the whole method is deeply suspect but it is also easy to use to convince patients. Forv that it makes perfgect sense. We sneeze, we cough, we then infect others.
Except when real science is applied we literally lose the argument over and over. The bizarre apparent success of the cow pox vaccine has now morphed into a couple of dozen protocols all lacking reliability or testability except plenty of manipulated stats.
It has finally been applied to so called virus based diseases which almost by definition cannot succeed. All to get governments to pay for global vaccination.
The Dogma and History of Vaccination. Questioning “Germ Theory” Is a Taboo
Global Research, August 22, 2022
\\
The problem with Covid vaccination is the problem with all vaccinations. All governments, and indeed almost everybody, but with significant exceptions, have accepted the germ theory and proceeded with vaccination in the face of monstrous failure and ineffectiveness.
But to question the germ theory and vaccination is like, in an earlier era, questioning the centrality of the earth in the universe. However, as was the case then, there is very good evidence for doing so.
The germ theory is primarily the result of the work of Louis Pasteur, Edward Jenner, and Robert Koch. If someone reads the book Béchamp or Pasteur by Ethel Douglas Hume, the work of Pasteur must come into question. Koch is renowned for his work on anthrax and tuberculosis, yet his vaccinations often resulted in disaster. Jenner in his own words has been caught trying to hide deaths resulting from his vaccinations.
Many Doctors and other scientists have raised questions about the germ theory in the past only to be vilified. For example Dr. Charles Creighton, generally considered the father of British epidemiology was asked to write the Encyclopedia Britannica article on vaccination, but decided to research the matter and come to his own conclusions:
“It is difficult to conceive what will be the excuse made for a century of cowpoxing; but it cannot be doubted that the practice will appear in as absurd a light to the common sense of the twentieth century as bloodletting now does to us. Vaccination differs, however, from all previous errors of the faculty, in being maintained as the law of the land on the warrant of medical authority. That is the reason why the blow to professional credit can hardly help being severe, and why the efforts to ward it off have been, and will continue to be so ingenious.”
Or let us take Lord Lister.
“Joseph Lister, 1st Baron Lister, OM, PC, PRS, FRCSE, FRCP Glas (5 April 1827 – 10 February 1912[1]) was a British surgeon, medical scientist, experimental pathologist and a pioneer of antiseptic surgery[2] and preventative medicine. Joseph Lister revolutionized the craft of surgery in the same manner that John Hunter revolutionized the science of surgery.[3]”
Lister was originally a supporter of Pasteur’s ideas, but through his work he was forced to change his mind and reject the possibility of airborne infection.
What was Lord Lister’s final judgment, after having abandoned the method into which he was misled by Pasteur? Here are his own words, as quoted by Dr. George Wilson:
“The floating particles of the air may be disregarded in our surgical work, and, if so, we may dispense with antiseptic washing and irrigation, provided always that we can trust ourselves and our assistants to avoid the introduction into the wound of septic defilement from other than atmospheric sources.”
Koch achieved immortal fame by isolating the tubercle bacillus in 1882 and the cholera vibrio the following year. He got the Noble Prize. However. Dr J.W. Browne, Medical Superintendent of the Kalyra Sanatorium, South Australia says:
“To date, upwards of two hundred different forms of tuberculin have been prepared and described.
The simple fact of the matter is that no one has yet been able to repeat Koch’s experiment successfully. There is no evidence but Koch’s in favour of tuberculin as a therapeutic cure for tuberculosis in guinea pigs, in calves, or in man. No one but Koch has been able to cure an infected guinea pig by the use of tuberculin of any sort.
Koch, as Shera says, was an optimist. There is no question that tuberculin can do infinite harm. Scores of people have died prematurely at its hands.
Never was there such a commercial vaccine as this one, and never has there been such a gigantic hoax. Tuberculin, Shera says, should not come within the range of vaccine therapy. Whatever good results are imputed to tuberculin must have occurred in spite of it, for its virtues are founded on experiments which cannot be repeated.
The disbeliever too, can point to many cases where the administration of tuberculin in pulmonary disease has been undoubtedly followed by disaster and, while he freely admits the undoubted powers of the tuberculin therapist to stir up the embers and kindle the fire, he has hitherto asked him in vain for any evidence of power to extinguish the fire.”
Herbert Shelton in Orthopathy describes many attempts to induce diseases by giving subjects germs supposedly known to cause them in food, swabs, and even injections without inducing any disease. He mentions the case of the murderer, Dr. Waite, and his victims, Colonel and Mrs. Peck. Waite tried at first to kill Mrs. Peck by giving her a disease. Here is an account of it written buy Lisa Mullenneaux.
As a fake physician, he had access to laboratory cultures from sources such as the Rockefeller Institute for Medical Research and the Cornell Medical Center. Detectives later found hidden in his apartment hundreds of test tubes and glass slides with labels such as “typhoid,” “diphtheria,” “pneumonia,” “tetanus,” and “asiatic cholera.” Disgustingly, the old lady refused to sicken when Waite added germs to her soup…”
No one has ever been able to induce disease through airborne infection. The theory of infectious, airborne disease, though as entrenched in the mind as once was the belief of the centrality of earth in the universe, does not stand up to scrutiny, and without it the efficacy of vaccines also disappears. But since vaccines often insert decayed biological substances or other toxic materials directly into the bloodstream, they can and often do cause diseases themselves. These diseases are not restricted to those the vaccine was intended to cure. This too is abundantly documented.
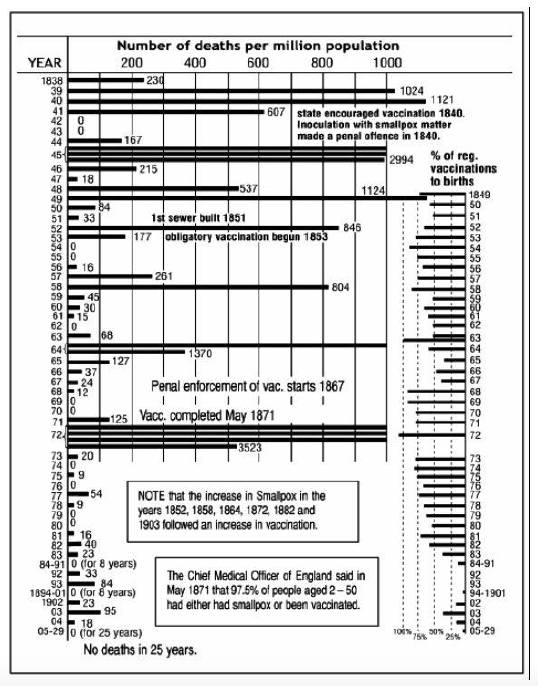
Here is an example of a vaccine associated with an increase in the disease it was supposed to prevent, small pox. This is a chart for the city of Leicester
As noted, vaccination became compulsory in 1840 and again in 1867. But in 1845 there was a huge outbreak of smallpox. By 1871 97.5% of the population had been vaccinated. Yet in 1872 3523 cases were recorded, the largest number by far in any year.
Dr R. Garrow, Medical Officer of Health for Chesterfield, England, asks why it is that the case mortality rate from smallpox in all persons over the age of 15 in England and Wales for the years 1923-6 was five times as high in the vaccinated (0.3%), as in those who were unvaccinated (0.06%)! He used official figures, and calculated only to one and two decimals; when figured to four decimals the rates become 0.324% and .0578%, nearer six times, the ratio between them being 5.6055 to 1.
Or again, in January 1899, Chief Surgeon Lippencott of the U.S. Army, writing from Manila, said: “The entire Command has been vaccinated at least four times since the appearance of the disease (smallpox).”
In the following March, he wrote again to state that all danger was over. However, in the reports of the Surgeon-General of the U.S.A. Army are to be found the following figures of smallpox cases and deaths:
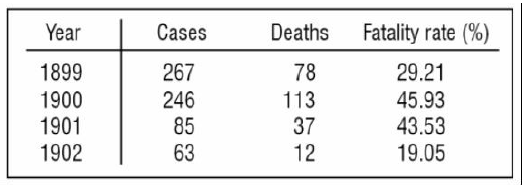
During the same period, the smallpox fatality rate among the far less vaccinated general population of the United States did not exceed 3%!
Pasteur’s first claimed success was with anthrax. Paul de Kruff in Microbe Hunters gives this account of Pasteur’s work on anthrax as evidence that even the great man can sometimes slip up.
“But one of Pasteur’s most charming traits was his characteristic of a scientific Phoenix, who rose triumphantly from the ashes of his own mistakes … so it is not surprising to find him, with Reux and Chamberlain, in 1881 discovering a very pretty way of taming vicious anthrax microbes and turning them into a vaccine…”
“Gradually, hardly a year after the miracle of Pouilly-le-Fort, it began to be evident that Pasteur, though a most original microbe hunter, was not an infallible god. Disturbing letters began to pile up on his desk; complaints from Montpotheir and a dozen towns of France, and from Packisch and Kapuvar in Hungary. Sheep were dying from anthrax – not natural anthrax they had picked up in dangerous fields, but anthrax they had got from those vaccines that were meant to save them! From other places came sinister stories of how the vaccines had failed to work – the vaccine had been paid for, whole flocks of sheep had been injected, the farmers had gone to bed breathing ‘Thank God for our great man Pasteur’, only to wake up in the morning to find their fields littered with the carcasses of dead sheep, and these sheep – which ought to have been immune – had died from the lurking anthrax spores that lay in their fields.
And this from a Pasteur cheerleader.
As mentioned earlier, vaccination is often associated with diseases other than the one it was meant to prevent. In 1881, the Sanitary Commission of the Hungarian Government said of the vaccine viruses used in the anti-anthrax inoculation:
“The worst diseases, pneumonia, catarrhal fever, etc., have exclusively struck down the animals subjected to injection. It follows from this that the Pasteur inoculation tends to accelerate the action of certain latent diseases and to hasten the mortal issue of other grave affections.”
In 1888 an institute in Odessa, Russia, sent some anti-anthrax vaccines to Kachowka in southern Russia, where 4,564 sheep were soon vaccinated, and 3,696 of them promptly turned up their toes and died; a death rate of 81 percent, and from a supposed ‘preventative’ vaccine at that!
The Zoophilist for May 1st 1891 reported deaths in 123 ‘selected’ cases [of tuberculosis] in Berlin from November 1890 to February 1891 which caused Koch to fall ‘under a cloud’, but he did not give up until the government finally closed him down because of the terrible death rate!
The Chief of the Bureau of Animal Industry of the US. Department of Agriculture says in his report for 1902:
“Most veterinary text books state that foot and mouth disease is a mild infection and that only 1 or 2 percent of the animals attacked die from it, the reader being left to infer that the losses do not exceed 2 or 3 percent of the value of the animals. Such a conclusion would be a grave mistake.”
However, it seems to have been mild before its cause was traced to vaccines. The Secretary of Agriculture says in the department1914 Year Book, page 20:
“There were outbreaks of foot and mouth disease in this country in 1870, 1880, 1884, 1902, and 1908. Since the close of the fiscal year 1914, the sixth outbreak has occurred. The first three, those of 1870, 1880 and 1884 were comparatively trifling. Those in 1902 and 1908 were more grave. The present one is the most serious and extensive of all.
In 1902, the outbreak occurred in the New England States. In 1908 it originated in Detroit. The origin of each of these new outbreaks was traced to the importation of vaccine virus for the propagation of vaccine for use in vaccinating people against smallpox. The vaccine was imported from Japan where the foot and mouth disease exists. Each of these outbreaks was stamped out by methods which have proved most effective in preventing the disease from gaining a footing. These methods involved the killing of all infected and exposed animals, the burying of the carcasses, and the thorough disinfection of all premises with which the animals may have come in contact.”
The first part of the 1914 outbreak was ascribed to ‘an imported article used in tanning’ (hides?) but when this was stamped out, a recurrence occurred near Chicago, in August 1915, that was traced to a Chicago laboratory making hog-cholera vaccines. Foot and mouth disease was found in 8 of 11 herds that had used this vaccine.
The Secretary of Agriculture says of this in the1915 Year Book (p.27):
“It seems certain that this infection was produced by contaminated hog-cholera serum prepared in Chicago, in October 1914, at an establishment where the disease had not been known to exist at any time.
…pending investigation, all shipments of serum from Chicago were prohibited. It was found that some of the product of the establishment had been used on 11 herds of hogs.
…infected hogs were found in eight of the herds and all 11 herds were slaughtered at once.”
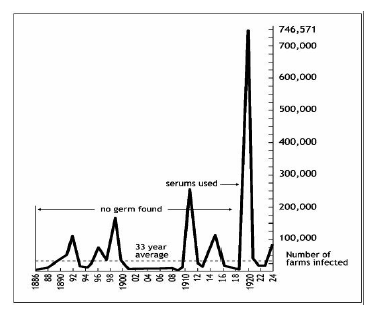
The Foot and Mouth Disease Commission of the U.S. Department of Agriculture published a chart showing the trend of foot and mouth disease in Germany from 1886 to 1924, which is reproduced below. Note the tremendous increase in deaths that accompanied the first general use of serums in 1920.
The Department’s Farmers’ Bulletin No. 666 says:
“Foot and mouth disease has prevailed in Europe for a great many years and has occasioned tremendous economic losses there. In Italy, France, Switzerland, Germany and Russia the plague has existed so long and has gained such a foothold that it is economically impossible to fight it with the American methods of slaughter and disinfection.”
Italy, France, Germany and Switzerland have compulsory vaccination, hence large vaccine plants that can spread the disease, as occurred in the cases cited in the United States. And of course neighbouring states with or without compulsory vaccination would be overrun by importation from these countries, though some, such as England, kept it out pretty well.
Other places where vaccination is pushed, such as Brazil, also have the disease, while Canada, the United States, Mexico, Australia and New Zealand, all of which are comparatively free from intensive vaccination drives, also seem to have only sporadic attacks of foot and mouth disease, which are generally easily stamped out.
How can the ‘scientists’ account for this?
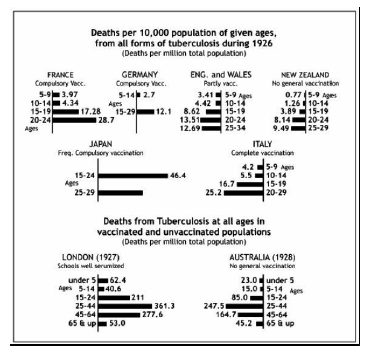
Here is a chart Parsons, in Pasteur: Plagarist, Imposter, shows that compares Tuberculosis rates in countries with heavy vaccination with those with less or none.
In the past, from time to time, the disaster of vaccination became obvious to nearly everyone except, of course, doctors and government officials.
The growing feeling for anti-vaccination reached full force in the 1890s with the National Anti-Vaccination League. The group organized protests and produced its own publications to distribute anti-vaccine propaganda. Ultimately, the voices of the anti-vaccination movement became too loud for the government to ignore and the government made it possible for people to opt-out of vaccination.
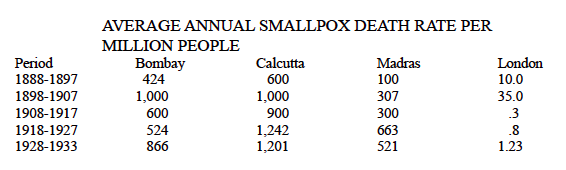
Around 1900, after the improvements in health due to sanitation and nutrition had had time to be weighed against that of vaccination, most of the people of England began to refuse vaccination, which resulted in a greater decline in smallpox, but in certain cities of India the British government was still able to keep up rigid enforcement. The following chart shows the high smallpox death-rate in three of these Indian cities as compared to the decreased death-rate in London after the clean up (health) campaign:
Perhaps the biggest vaccination success is the eradication of polio. Salk vaccine was introduced in 1955 and by 1962 polio was all but gone. But Post hoc ergo propter hoc is a logical fallacy that states: “Since event Y followed event X, event Y must have been caused by event X.” Other important events happened during this time. In particular DDT production and use declined dramatically.
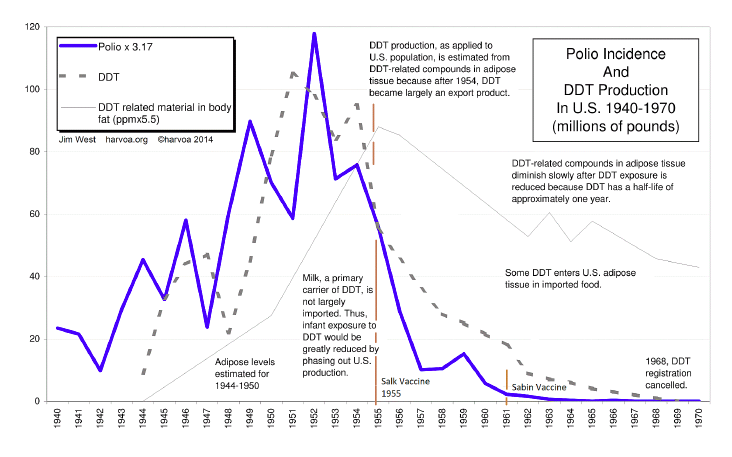
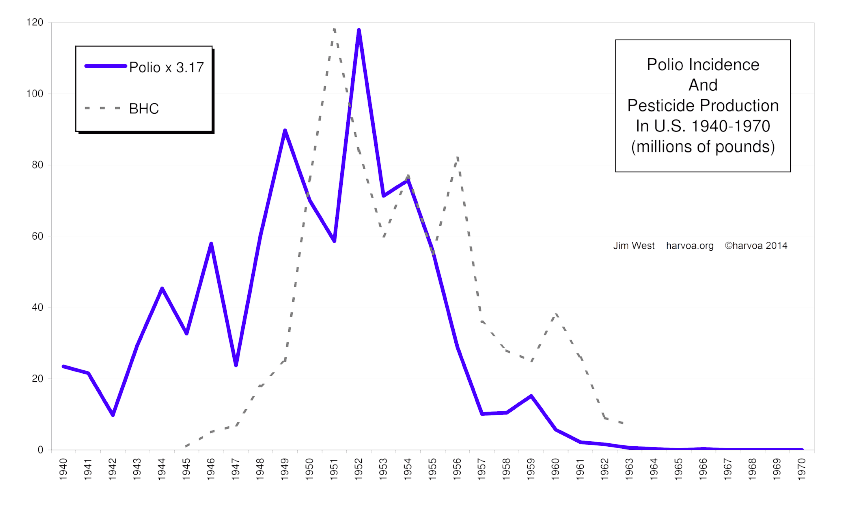
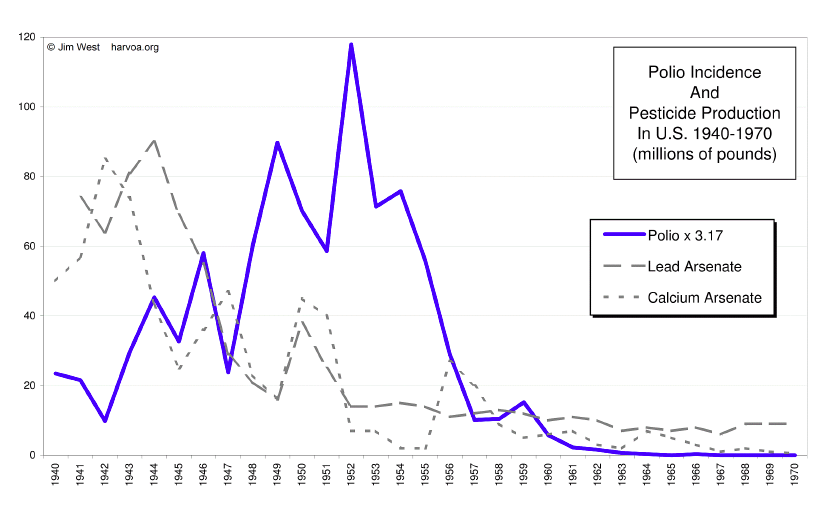
Other pesticides were also heavily used in this period. BHC was known to cause fatalities. Arsenic compounds were also heavily used and were withdrawn during this period. Although DDT lagged behind polio incidence in the early 40’s, other arsenides were used heavily.
The connection between DDT and polio was more than just coincidental. Mortan Biskind’s research discovered this connection almost immediately.
Particularly relevant to recent aspects of this problem are neglected studies by Lillie and his collaborators (74, 75) of the National Institutes of Health, published in 1944 and 1947 respectively, which showed that DDT may produce degeneration of the anterior horn cells of the spinal cord in animals. These changes do not occur regularly in exposed animals any more than they do in human beings, but they do appear often enough to be significant. When the population is exposed to a chemical agent ‘known to produce in animals lesions in the spinal cord resembling those in human polio, and thereafter the latter disease increases sharply in incidence and maintains its epidemic character year after year, is it unreasonable to suspect an etiologic relationship?
But polio research focused almost exclusively on seeking a viral cause.
*
The evidence for corruption and obvious deception among vaccination’s proponents is ample. John Baron, in his Life of Jenner quotes Jenner,
“‘When I found Dr. Woodworth about to publish his pamphlet relative to the eruption (smallpox) cases at the Smallpox Hospital, I entreated him in the strongest terms, both by letter and conversation, not to do a thing that would so disturb the progress of vaccination.”
Thomas Morgan in his Medical Delusions writes,
“Jenner soon discovered that vaccination did not give immunity from smallpox, including some who had been vaccinated by himself and had died from it. Not wishing to bring vaccination into disrepute, he endeavored to suppress reports, and in writing to a friend, said, ‘I wish my professional brethren to be slow to publish fatal results after vaccination.”
Pasteur’s questionable practices are well documented in Béchamp or Pasteur.
At home, too, there were annoyances. At the Academy of Medicine, voices were raised against the germ theory of disease, and in particular M. Peter ridiculed Pasteur’s all-conquering microbe. It was easy for him to do this, as in March 1882 the reputation of the vaccine for anthrax had met with a disastrous downfall.
It had come about in this way; in Italy it had been thought worth while for a commission composed of members of the University of Turin to perform experiments such as Pasteur had described, and thus test his prophylactic. As a result, to quote René Vallery-Radot,
“All the sheep, vaccinated and unvaccinated, had succumbed subsequently to the inoculation of the blood of a sheep that had died of charbon.”
After about a year of dispute and passing the buck by correspondence, the Turin professors published a pamphlet in June 1883, containing some of Pasteur’s contradictory statements together with their cutting criticisms thereof, under the title Of the Scientific Dogmatism of the Illustrious Professor Pasteur, which was signed by six professors of high standing. This, by citing contradictory statements Pasteur had made in different papers, along with their comments, just about destroyed his theories on anthrax.
This paper was translated into French, but Pasteur, with some adroit dissimulation, managed to survive the blow, and went on pushing his anthrax vaccine.
Medical professionals of high repute seriously questioned and offered significant evidence against the germ theory and the program of vaccination. Creighton expected it to be long discredited, indeed incredible, by now. At the beginning of the nineteenth century medical education was unregulated and informal, and medical practice included a number of different approaches, but “preventive” medicine was not among them. How did “preventive” medicine and the universal acceptance of vaccination as its primary treatment become the orthodoxy it is today?
Industrialization in the nineteenth century required social and political transformations and the creation of a workforce from a recalcitrant population of farmers and craftsmen. E. Richard Brown in Rockefeller Medicine Men argues that
“corporate capitalists turned to philanthropy, the universities, and then to medicine to solve some of the many problems that grew out of capitalist industrialization… For the brief period from about 1900 to World War I science-oriented medical schools and the AMA joined forces to press for the acceptance of scientific medicine.”
Scientific medicine, insofar as it was preventive, was primarily adherence to the ideas of Jenner, Pasteur, and Koch. The Carnegie Foundation for the Excellence of Teaching and the Rockefeller foundation allied with the AMA before WW II to produce this result. Brown argues that these foundations did not manipulate medicine for financial gain, but to shape it to serve the new social structure of industrial capitalism rapidly developing by the end of the nineteenth century.
It was a time when the “trusts” had come under strong political pressure. Class war seemed to be in the cards. The super rich justified the new industrial society by arguing for its rationalism. Monopoly, because of the economy of size, was considered the rational organization of production. Social Darwinism justified ruthlessness. Science, it was argued, justified industrialism. Philanthropic successful capitalists supported charities to spur the poor to ameliorate their condition.
They financed Universities to encourage scientific education to produce the needed educated workforce. There was a need to prove that industrialism and its titans of industry were good. These concerns combined in an interest in medicine. ”This union of corporate philanthropy, the managerial professional stratum, and the universities in supporting science spawned the Rockefeller medicine men and their new system of medicine,” Brown argues.
Brown quotes Rockefeller:
The best philanthropy, the help that does the most good and the least harm, the help that nourishes civilization at its very root, that most widely disseminates health, righteousness, and happiness, is not what is usually called charity. It is, in my judgment, the investment of effort or time or money, carefully considered with relation to the power of employing people at a remunerative wage, to expand and develop the resources at hand, and to give opportunity for progress and healthful labour where it did not exist before. No mere money-giving is comparable to this in its lasting and beneficial results.
To make a long story short the conclusion was that scientific philanthropy must concern itself with “prevention rather than relief,” according to Amos Warner, a Stanford economist active in the movement.
The inclusion of science in university curriculum had already begun.
On the last day of April in 1846 Edward Everett, the new president of Harvard University laid before his inaugural convocation a proposal, that Harvard found a “school of theoretical and practical science” to teach “its application to the arts of life,” to furnish a “supply of skillful engineers” and other persons who would explore and develop the “inexhaustible natural treasures of the country, and to guide its vast industrial energies in their rapid development.”
The industrialist Abbott Lawrence underwrote the new school, and the push for sciences to be taught in the American universities grew apace. Now medicine came under this umbrella.
William H. Welch was a doctor who openly despised medical practice with patients and, after returning in 1878 from studies with Robert Koch in bacteriology in Germany, sought a university position as a pure researcher. He achieved that goal with, first, a position at Bellevue and, in 1884, a position at Johns Hopkins. In 1893 he became Johns Hopkins medical school’s first dean. Brown quotes Donald Fleming’s biography, William H. Welch and the Rise of Modern Medicine.
“In 1901 he [Welch] came to the attention of Frederick T. Gates, the grand master of the Rockefeller philanthropies. Welch was asked to help organize the Rockefeller Institute for Medical Research. He soon became chief adviser to the Rockefeller foundations on medical projects, assisting in important ways in funding medical education in the United States and China,..Under the skillful direction of foundation officers, the Rockefeller wealth became the largest single source of capital for the development of medical science in the United States, the conversion of medical education to a scientific research basis, and the development of public health programs in the United States and abroad.”
Brown continues:
By 1928 Rockefeller gifts to the institute totaled $65 million, an enormous sum for the period. Although the elder Rockefeller and his son are most widely known for the benefactions, it was Frederick T. Gates who formulated the strategies and initiated the investments in medical research, medical education, and public health.
Gates, in his memoir recounting how he came to the project tells of a minister who recommended the work of William Osler, which Gates obtained and read in one night.
When I laid down this book, I had begun to realize how woefully neglected in all civilized countries and perhaps most of all in this country, had been the scientific study of medicine. I saw very clearly also why this was true. In the first place, the instruments for investigation, the microscope, the science of chemistry, had not until recently been developed. Pasteur’s germ theory of disease was very recent. Moreover, while other departments of science, astronomy, chemistry, physics, etc., had been endowed very generously in colleges and universities throughout the whole civilized world, medicine, owing to the peculiar commercial organization of medical colleges, had rarely if ever, been anywhere endowed, and research and instruction alike had been left to shift for itself dependent altogether on such chance as the active practitioner might steal from his practice.
That July Gates dictated a memorandum to Rockefeller pointing out the usefulness of the Koch and Pasteur Institutes. Although it took several years, partially because Rockefeller senior supported homeopathy against his son and Gates who were advocates of “science,” the Rockefeller Institute for Medical Research began its work in 1901 with Dr. Simon Flexner, one of Koch’s students, as its executive director. Brown grants that Gates had genuine humanitarian motives, but was primarily influenced by Simon Flexner and William Welch, both students of Koch. Brown quotes Gates from Some Elements of an Effective System of Scientific Medicine in the United States that “the fundamental aim of medical science ought to be not primarily the cure but primarily the prevention of disease.” Naturally he was inclined to support preventive vaccination.
Medical scientists, when they returned from scientific study in Europe, got prestigious faculty jobs in the new university departments. Johns Hopkins was staffed almost entirely with students who had studied in Germany. These were the people, rather than the clinicians who actually saw patients, that the Philanthropists turned to.
At the turn of the century the scientists joined with elite practitioners to gain control of the AMA where they worked to introduce more elaborate and expensive educational requirements and so reduce the number of lesser practitioners. Reformers within the AMA used the technical requirements to set standards which more and more favored laboratory scientists and students of substantial means at the expense of clinical practitioners and poorer, however talented, students.
The AMA was founded in 1847 as a trade association whose purpose was to serve the interests of doctors, but was essentially ineffective until 1901 when it was reorganized under Dr. George H. Simmons who, though educated in homeopathy later rejected it. Simmons increased the power of the AMA by creating a hierarchical representative structure and strengthening the local societies. Brown quotes the committee on reorganization that its intention was “to foster scientific medicine and to make the medical profession a power in the social and political life of the republic.”
“From its founding onward, the AMA was hostile to the interests of proprietary medical colleges and their faculties. The practitioners [AMA] wanted to reduce the output of medical schools in order to reduce competition within the profession, while the medical faculties opposed any attempted reforms because of their interests in maximizing their lecture fees and future consulting fees…
Within two years the state medical societies, under the guidance of the Council on Medical Education, dominated the state boards. Through the influence of the state societies and direct contact by the council, the licensing boards increasingly became agents of the council’s plan of action.
Once in control of the reorganized AMA and the state boards in charge of licensing, the reformers launched their most effective tool for transforming the profession. In 1904 the AMA replaced its temporary committee on medical education with a permanent Council on Medical Education, headed by the energetic and resourceful Arthur Dean Bevan, The council inspected every one of the country’s 160 medical schools and gave them grades primarily on their scientific facilities and requirements for entrance.
In 1907 Bevan had invited Henry S. Pritchett, president of the Carnegie Foundation for the Advancement of Teaching, to examine the survey materials collected by the council. Bevan convinced Pritchett of the value of a Carnegie supported study of medical education. Pritchett discussed the proposed study with Charles Eliot, president of Harvard and a trustee of the Carnegie Foundation, Rockefeller’s General Education Board, and the Rockefeller Institute for Medical Research. He also talked with Dr. Simon Flexner, a Koch student and director of the Rockefeller Institute. Flexner suggested a director for the study, his brother Abraham.
Abraham Flexner was not a doctor, and when he met with Pritchett he told him so, but Pritchett assured him that he wanted a layman for the job, not a doctor. In any case Abraham Flexner was in no position to judge the science in “scientific” medicine. In his Autobiography Flexner reveals himself as a fanboy of great minds.
Pasteur, Lister, Koch, Ehrlich, and an unending line of physicists and chemists had their feet in both worlds—the world of practice and the world of theory. Minds that are fundamental in their searching, whatever the spring that moves them…
He describes his preparation for his task.
Having finished my preliminary reading, I went to Baltimore—how fortunate for me that I was a Hopkins graduate!—where I talked at length with Drs. Welch, Halsted, Mall, Abel, and Howell, and with a few others who knew what a medical school ought to be, for they had created one. I had a tremendous advantage in the fact that I became thus intimately acquainted with a small but ideal medical school embodying in a novel way, adapted to American conditions, the best features of medical education in England, France, and Germany. Without this pattern in the back of my mind, I could have accomplished little. With it I began a swift tour of medical-schools in the United States and Canada—155 in number, every one of which I visited.
According to Brown the Carnegie imprimature suggested future support for schools Flexner approved of in his famous Flexner Report and the competition for students made schools all fear bad publicity for those he didn’t. For whatever reason almost all schools opened themselves to Flexner’s inquiry.
“If many competing medical schools that cooperated with the Carnegie study got a large advantage—for example, a new laboratory or an endowment—the financial collapse and demise of the disadvantaged was assured.”
By 1910 the number of schools had fallen from a high of 166 to 131. With AMA domination of the state licensing boards it was impossible for a student in a downgraded school to get licensed, and so those schools failed. Schools embraced the germ theory and vaccination or else.
Superfluous educational requirements justified by “science” and especially the germ theory served the aims of the AMA by reducing the number of practitioners. “From the moment it opened its doors in 1893, Johns Hopkins medical school led the way by requiring a bachelor’s degree for admission and four years of instruction for its prestigious M.D. degree. When Harvard instituted the baccalaureate requirement in 1901, its entering medical class dropped from an all-time high of 198 students the previous year to sixty-seven.”
To limit the number of doctors the AMA sought to make Medicine a “profession.”
Eliot Freidson [a theorist on professions] has observed, any occupation wishing professional status creates a systematic body of theory, claims exclusive authority of its practitioners, adopts a code of ethics, tries to build solidarity among its practitioners around formal values, norms, and symbols, and otherwise cloaks itself with the well-known medallions of professions to support its claims. “If there is no systematic body of theory,it is created for the purpose of being able to say there is.”
What the medical reformers sought was the power to enforce the instruments of professionalism that assure high incomes, social status, and continued prosperity for the profession.”
A profession has a code of “ethics.” The AMA code of ethics gave doctors unquestioned authority over medical decisions. “”The obedience of a patient to the prescriptions of his doctor should be prompt and implicit,” the code of ethics instructed. The patient “should never permit his own crude opinions as to their fitness to influence his attention to them.” The code of ethics also forbids a doctor from commenting on the practices of another. The confidentiality of medical records prevents criticism of medical practice by other doctors. The AMA realized that to become a profession medicine had be become a “science” with “an ideology and a practice that was consistent with the ideas and interests of socially and politically dominant groups in the society.”
Being a “science” was in opposition to being a science. Although these institutions called themselves scientific, the education they provided, and provide today is anything but. John L. Spivak in The Medical Trust Unmasked quotes Dr. David L. Edsall, then Dean of the Harvard Medical School:
“Almost all subjects must be taken at exactly the same time and exactly the same way by all students and the amount introduced into each course is such that few students have the time and energy to explore any subject in the spirit of independent interest… A little comparison shows that there is less intellectual freedom in the medical course than in almost any other form of professional education in this country.”
It is no wonder that the germ theory, so obviously faulty, could be so casually accepted and those who question it called crackpots. Anyone who objected couldn’t get licensed. Dr. Edsall continues:
“I was, for a period, a professor of therapeutics and pharmacology, and I know from experience that students were obliged then by me and by others to learn about an interminable number of drugs, many of which were useless, some probably even harmful, some others relatively valueless, because they were still discussed in some text books, which had never been officially discarded and were sometimes asked about by State Boards of Medical Examiners.”
These are the words of an authority upon this subject, not only about machine-made doctors, but about the control that the medical examining board, themselves controlled by the AMA with its restrictive agenda, has upon the medical curriculum. The germ theory fit the needs of both the AMA and the philanthropists. Brown comments,
“The germ theory of disease was especially attractive to both the regular profession and these new industrial and corporate elites. The germ theory emphasized discrete, specific, and external causal agents of disease. It gave encouragement to the idea of specific therapies to cure specific pathological conditions. The payoff for the medical practitioners would be increased technical effectiveness and improved standing in the eyes of the public….Disease was thus seen as an engineering problem, surmountable with sufficient talent and resources… Scientific medicine wrapped the modern doctor in an aura of therapeutic effectiveness, and the limited improvements gave support to that aura.”
In summary, by the beginning of the twentieth century embracing “scientific” medicine was a requirement for medical licensing, forcing out homeopathy, chiropractic and other practices even though, as we have seen, it was not having therapeutic success and experiencing frequent disasters. But the philanthropists, whose interests the theory served, could not judge of the quality of the therapy and the “scientists” had vested interests in burying unpleasant news. The use of “science” to restrict entry into the profession satisfied the AMA for it was the ideal tool to control licensing. But the adoption of “science” had nothing to do with science.
The discrediting of Peter Duesberg for questioning the connection between AIDs and HIV, even though there is no experimental evidence of this connection, proves that this censorship is, if anything, even more virulent today. This victory should not be attributed to any ulterior motives on the part of the philanthropists. Although they were men of business, ravenous for profit, I have found no evidence that they thought they were doing anything but good, though their idea of good, the shaping of society for the benefit of industrialism, could be questioned. But these motives, praiseworthy or not, were not those that should motivate science.
The motives of Pasteur, Koch, and the other “scientists” are less pure. There is no doubt that desire for fame and fortune clouded their judgment and led them to suppress unfavorable results including vaccine related deaths. Interestingly Welch, in Munich, found a man Named Max von Pettenkofer who had ideas very much like those of today’s terrain theorists. But this did not suit the ambitious Welch. In my opinion corruption is an almost inevitable result of the commercialization of science. A scientist hoping to make a killing will inevitably be tempted to suppress any evidence of his failure and denigrate the successes of opponents. There is plenty of evidence that these men did so. Flexner was notorious for refusing to finance any experiments that might bring the germ theory into question. Today it is said that up to 80% of the experiments published by The Lancet are not reproducible. The commercialization of science undermines a scientist’s necessary objectivity. One need only gaze upon the deplorable behavior of drug companies.
Béchamp, ignoring the forces allied against him, attributed Pasteur’s theoretical victory to the simplicity of his theory. Two microscopic armies contending within the body is easy to imagine. One might wonder that so many experiments that seem to confirm the germ theory could yet be so wrong. This is a product of the ignorance about the difference between Béchamp’s theory and Pasteur’s.
Pasteur argued that bacteria were invaders from outside met by antibodies created by the human body to defeat them. Disease was a result of a loss by the home team. Vaccination provided a skirmish that the home team could more easily win and in the course would cause it to produce specialized weapons, antibodies, that would be ready should another encounter with the same enemy occur.
Béchamp thought disease was a crisis in the body’s ability to eliminate toxins, which is usually handled by unnoticed routine. Vomiting, excess mucus, diarrhea, skin eruptions,and fever are ways that the body in crisis eliminates toxins. Disease is the body’s response to a crisis and should not be inhibited. Bacteria, produced by the body itself, are part of the normal mechanism of toxin removal. There are also alien bacteria that have a similar function outside — to turn organic waste, dead matter, into a form that could then be taken up by new life. They are an essential element of the life cycle. If outside bacteria enter the body they do not reproduce there and are treated by the body like any other toxin, and like any other toxin can produce inflammation and disease, but do not commandeer cell mechanisms to reproduce themselves. This rarely happens in any serious way unless the body’s protective barriers— skin, mucus membrane, stomach acid– is bypassed as it is with vaccination or wounds.
So in both theories bacteria would be present in sites of disease. Experiments that found bacteria at such sites would be consistent with both theories, and the experiments mistakenly thought to confirm the germ theory were such experiments. It is sometimes said that constant conjunction does not prove causation, but this is logically incorrect. Constant conjunction does prove causation but not the direction of causation. Advocates of Béchamp offer the analogy of fire trucks always at fires but not the cause of them. In this case the fires are the cause of the presence of the trucks. Constant conjunction shows that one thing is the cause of another but not which in the cause which the effect, or that both have a third common cause. Common conjunction cannot determine which of these three possibilities obtains.
Alien bacteria, like any other toxin could, if they managed to pass the body’s barriers, cause a toxic crisis, though it might not look like the one germ theorists have associated with it. They might even have been seen to have done the damage. But they are a toxin and do not reproduce in the body. On the other hand the body’s own bacteria might appear to reproduce within cells, but these would be cells already damaged or dead. These bacteria are beneficial and do no damage. They eliminate toxins, which includes the body’s own damaged cells.
That vaccinations are associated with diseases different from those they were meant to prevent is well documented. Swelling and reddening around vaccination sites is routine, though such reactions might not be one of the symptoms associated with the specific disease. Florence Nightingale, the famous nurse, insisted that there were no specific diseases, and that those who were ill exhibited symptoms of many supposedly separate diseases during the course of the illness. Béchamp demonstrated that bacteria could change their shape in response to the toxins present.
One experiment Bechamp performed was to bury a dead cat in sand in a container and seal the container. When he opened it he found bacteria below the cat but not above, seeming to prove that the bacteria did not get into the container afterwards through the lid. This should be an easy test for the external entrance of bacteria or the body’s ability to produce them itself.
Since the 1990’s the presence of the microbiome has become accepted. We now all recognize the presence of “good bacteria” in the digestive tract that aid digestion by consuming indigestible fibre. That is, they do just what Béchamp said they did. Experiments have cleanly shown that the microbiome is unique to each individual.
“The results showed that the codes were unique among hundreds of individuals, and that a large fraction of individuals’ microbial “fingerprints” remained stable over a one-year sampling period.”
If so how can these bacteria have come from outside?
What about epidemics?
THE devastating Black Death which killed hundreds of millions of people in the 14th century may have been triggered by an asteroid impact, scientists have sensationally claimed. By NATHAN RAO
The Black Death may have been triggered by asteroid impact
The shocking revelation threatens to debunk one of the biggest chunks of British history and turn the world of science and academia on its head….
It is widely accepted that the 14th century epidemic, the most catastrophic ever recorded in Europe’s history, was a caused by the bacteria Yersinia pestis which spread from China. However experts now claim something “much bigger” happened at the time to kill off 60 per cent of the population.
Author and dendochronologist Professor Mike Baillie said studies of tree rings reveal a major event just before 1350, just at the time the disease was sweeping across Europe.
Something catastrophic occurred to change the composition of the atmosphere and provide ideal conditions for a lethal infection to spread, he claims.
The great influenza pandemic of 1918-19 has no easily provable explanation, but there are several possible factors that do not involve a virus. First, of course, is the Great War, with its gas attacks and horribly unsanitary trenches. Then, one of the strongest ENSO incidents of the twentieth century occurred during those same years and contributed to famines, floods, and the spread of malaria. And finally, of course there were increased vaccination of troops and others during the war. In any case the description of the spread of the pandemic through contagion is pure conjecture without any possibility of evidence.
Ralph R. Scobey, M.D. offers a wealth of evidence of a toxic origin of polio. Here is a comparison of polio incidence and pesticide production.
How about Malaria? “Malaria is caused by Plasmodium parasites. The parasites are spread to people through the bites of infected female Anopheles mosquitoes, called ‘malaria vectors’.” Although Anopheles mosquitoes and Plasmodium parasites exist on every continent except Antarctica, malaria is restricted to tropical regions. However, during the fifteenth century malaria was found in parts of England. This included a period known as “the little ice age” during which England was considerably colder than it is now. However, the CDC web page entitled Where Malaria Occurs states that, “Temperature is particularly critical.”
Germ theorists claim that some people get ill in a pandemic while others don’t because of the varying strengths of immune systems. But people with strong immune systems are invariably those who are healthy in general. People who eat properly, get sufficient exercise, and live in sanitary conditions will have strong “immune systems.” But this is just the terrain theory by another name. To say someone has a strong immune system is to say they are healthy. All we have to do is realize that this is what is important, not germs. Vaccines, bypass the bodies barriers to insert toxins, and damage general health. Of course there is not much profit in encouraging healthy living.
Were preventive medical practice truly scientific these considerations should raise questions about the germ theory and vaccination, but because the highly profitable theory is unscientifically held as a truth universally accepted, and those who question it held as crackpots, they don’t.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Michael Doliner studied with Hannah Arendt at the University of Chicago and taught (awhile ago) at Ithaca College and Valparaiso University. He has a degree in Mathematics.
Featured image is from NaturalNews.com
The original source of this article is Global Research
Copyright © Michael Doliner, Global Research, 2022
No comments:
Post a Comment