
In the face of ample real science the test is set to produce a massive number of false positives. This is useless. worse than that it cannot separate out dead virus remnants from live viruses.
What are they thinking except to promote a pandemic scare in order to sell vaccinations willy nilly.
The problem does not end there. It appears the purpose of the vaccine is to introduce Specific RNA remnants which then make us vulnerable to the real COV 19 infection itself.. This is a complete reversal of the vaccine MEME.
This really looks more and more an act of WAR. The first roll out in Wuhan will have been through a Vaccine. When the deaths began sometime later during the natural flu season, they claimed a novel virus.
This is ugly.
ASTONISHING COVID-19 TESTING FRAUD REVEALED
January 13, 2021
Get the latest Waking Times articles delivered to your inbox. Sign up here.
Dr. Mercola, Guest
https://www.wakingtimes.com/astonishing-covid-19-testing-fraud-revealed/
The COVID-19 pandemic has brought us many harsh lessons. Importantly, it has shown us how easy it is to manufacture panic and control entire populations through deceptive means. Topping the list of deceptive strategies is the use of a test that falsely labels healthy individuals as sick and infectious. This allows mass testing to drive the narrative that we’re in a lethal pandemic.
Of course, I’m talking about the now infamous reverse transcription polymerase chain reaction (RT-PCR) test. The fact is, the PCR test is not designed to be used as a diagnostic tool as it cannot distinguish between inactive viruses and “live” or reproductive ones.1
This is a crucial point, since inactive and reproductive viruses are not interchangeable in terms of infectivity. If you have a nonreproductive virus in your body, you will not get sick and you cannot spread it to others. Secondly, many if not most laboratories amplify the RNA collected far too many times, which results in healthy people testing “positive.”
The Crucial Detail That Nullifies Most PCR Test Results
The video above explains how the PCR test works and how we are interpreting results incorrectly. In summary, the PCR swab collects RNA from your nasal cavity. This RNA is then reverse transcribed into DNA. Due to its tiny size, it must be amplified to become discernible. Each round of amplification is called a cycle, and the number of amplification cycles used by any given test or lab is called a cycle threshold (CT).
The higher the CT, the greater the risk that insignificant sequences of viral DNA end up being magnified to the point that the test reads positive even if your viral load is extremely low or the virus is inactive and poses no threat to you or anyone else.
Many scientists have noted that anything over 35 cycles is scientifically indefensible.2,3,4 A September 28, 2020, study5 in Clinical Infectious Diseases revealed that when you run a PCR test at a CT of 35 or higher, the accuracy drops to 3%, resulting in a 97% false positive rate.
Yet, a test known as the Corman-Drosten paper and tests recommended by the World Health Organization are set to 45 cycles,6,7,8 and the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention recommend running PCR tests at a CT of 40.9
The question is why, considering the consensus is that CTs over 35 render the test useless. When labs use these excessive cycle thresholds, you clearly end up with a grossly overestimated number of positive tests, so what we’re really dealing with is a “casedemic”10,11 — an epidemic of false positives.
Many are now questioning whether this was done on purpose to crash the global economy and provide cover for the implementation of what’s known as the Great Reset, which is nothing less than a global totalitarian takeover by unelected technocrats who seek to gobble up all the world’s assets.
Indeed, it seems quite clear we’re not dealing with a lethal pandemic in any real sense. Mortality statistics further prove this is the case, as overall mortality statistics have remained stable in 2020 and in line with previous years.12,13,14
In other words, people are dying from COVID-19, yes, but the illness is not killing an excess number of people. The same number of people would have died anyway, from something. Indeed, CDC data15 released August 26, 2020, showed only 6% of so-called COVID-19 deaths had COVID-19 listed as the sole cause on the death certificate.
“For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death,” the CDC stated, and any one of those comorbidities could have killed those people even if COVID-19 was nonexistent.
For Accuracy, Much Lower CTs Must Be Used
Now, if CTs above 35 are scientifically unjustified, just how low of a CT should be used? Quite a few studies have investigated this, so there’s no shortage of data at this point. The fact that the WHO, FDA and CDC still have not changed their CTs downward in light of all these data tells us they’re not interested in getting an accurate picture of the infection rate.
For example, an April 2020 study16 in the European Journal of Clinical Microbiology & Infectious Diseases showed that to get 100% confirmed real positives, the PCR test must be run at 17 cycles. Above 17 cycles, accuracy drops dramatically.
By the time you get to 33 cycles, the accuracy rate is a mere 20%, meaning 80% are false positives. Beyond 34 cycles, your chance of a positive PCR test being a true positive shrinks to zero.
More recently, a December 3, 2020, systematic review17 published in the journal of Clinical Infectious Diseases assessed the findings of 29 different studies — all of which were published in 2020 — comparing evidence of SARS-CoV-2 infection with the CTs used in testing.
“Five of the studies included were unable to identify any live viruses in cases where a positive PCR test had used a CT above 24. What’s more, in order to produce live virus culture, a patient whose PCR test used a CT at or above 35 had to be symptomatic.“
As reported by the authors, “12 studies reported that CT values were significantly lower … in specimens producing live virus culture.” In other words, the higher the CT, the lower the chance of a positive test actually being due to the presence of live (and infectious) virus.
“Two studies reported the odds of live virus culture reduced by approximately 33% for every one unit increase in CT,” the authors noted. Importantly, five of the studies included were unable to identify any live viruses in cases where a positive PCR test had used a CT above 24. What’s more, in order to produce live virus culture, a patient whose PCR test used a CT at or above 35 had to be symptomatic.
So, to summarize, if you have symptoms of COVID-19 and test positive using a PCR test that was run at 35 amplification cycles or higher, then you are likely to be infected and infectious.
However, if you do not have symptoms, yet test positive using a PCR test run at 35 CTs or higher, then it is likely a false positive and you pose no risk to others as you’re unlikely to carry any live virus. In fact, provided you’re asymptomatic, you’re unlikely to be infectious even if you test positive with a test run at 24 CTs or higher.
Fearmongering Success Hinges on Incorrect Use of PCR Test
The video above includes several interviews with experts who have openly criticized the use of PCR testing to diagnose infections such as COVID-19. These include:
The inventor of the PCR test, the late Kary Mullis (he has spoken about the test for other infections, such as HIV, but died in August 2019, a few months before the COVID-19 pandemic broke out)
Michael Yeadon, Ph.D., a former vice-president and chief scientific adviser of the drug company Pfizer
Professor Carl Heneghan, director of the Oxford University Center for Evidence-Based Medicine
Emeritus professor of immunology Beda M. Stadler, former head of the Bern Institute of Immunology
Clare Craig, a consultant pathologist
Stephen A. Bustin, professor of molecular medicine and a world-renowned expert on the PCR test
In 1993, Mullis spoke about the use of the PCR test to diagnose HIV. He explained that all the test does is amplify molecules into something you can detect, but it cannot tell you whether those particles actually pose a risk to your health.
He also points out that, using PCR, you can essentially find just about anything in anyone because most of us are walking around with pathogens of all sorts, but the load is either too low to be of concern or the particles are just dead debris that pose no risk.
Bustin points out that when you get a positive result using a CT of 35 or higher, you’re looking at the equivalent of a single copy of viral DNA. The likelihood of that causing a health problem is minuscule. Even Dr. Anthony Fauci has admitted that using a PCR test with a CT above 35 renders it more or less useless because at that point, you’re just detecting dead nucelotides. No live virus can be detected at CTs that high.
Fatal Errors Found in Paper on Which PCR Testing Is Based
November 30, 2020, a team of 22 international scientists published a review18 challenging the scientific paper19 on PCR testing for SARS-CoV-2 written by Christian Drosten, Ph.D., and Victor Corman. The Corman-Drosten paper was quickly accepted by the WHO and the workflow described therein was adopted as the standard across the world.
According to Reiner Fuellmich,20 founding member of the German Corona Extra-Parliamentary Inquiry Committee (Außerparlamentarischer Corona Untersuchungsausschuss,21 or ACU),22,23 Drosten is a key culprit in the COVID-19 pandemic hoax.
The scientists demand the Corman-Drosten paper be retracted due to “fatal errors,”24 one of which is the fact that it was written (and the test itself developed) before any viral isolate was available. All they used was the genetic sequence published online by Chinese scientists in January 2020.
The fact that the paper was published a mere 24 hours after it was submitted also suggests it didn’t even undergo peer review. In an Undercover DC interview, Kevin Corbett, Ph.D., one of the 22 scientists who are now demanding the paper’s retraction, stated:25
“Every scientific rationale for the development of that test has been totally destroyed by this paper. It’s like Hiroshima/Nagasaki to the COVID test.
When Drosten developed the test, China hadn’t given them a viral isolate. They developed the test from a sequence in a gene bank. Do you see? China gave them a genetic sequence with no corresponding viral isolate. They had a code, but no body for the code. No viral morphology.
In the fish market, it’s like giving you a few bones and saying ‘that’s your fish.’ It could be any fish … Listen, the Corman-Drosten paper, there’s nothing from a patient in it. It’s all from gene banks. And the bits of the virus sequence that weren’t there they made up.
They synthetically created them to fill in the blanks. That’s what genetics is; it’s a code. So, its ABBBCCDDD and you’re missing some, what you think is EEE, so you put it in … This is basically a computer virus.
There are 10 fatal errors in this Drosten test paper … But here is the bottom line: There was no viral isolate to validate what they were doing. The PCR products of the amplification didn’t correspond to any viral isolate at that time. I call it ‘donut ring science.’ There is nothing at the center of it. It’s all about code, genetics, nothing to do with reality …
There have since been papers saying they’ve produced viral isolates. But there are no controls for them. The CDC produced a paper in July … where they said: ‘Here’s the viral isolate.’ Do you know what they did? They swabbed one person. One person, who’d been to China and had cold symptoms. One person. And they assumed he had [COVID-19] to begin with. So, it’s all full of holes, the whole thing.“
The conclusion of the review reads, in part:26
“A decision to recognize the errors apparent in the Corman-Drosten paper has the benefit to greatly minimize human cost and suffering going forward. Is it not in the best interest of Eurosurveillance to retract this paper? Our conclusion is clear. In the face of all the tremendous PCR-protocol design flaws and errors described here, we conclude: There is not much of a choice left in the framework of scientific integrity and responsibility.”
The critique against PCR testing is further strengthened by a November 20, 2020, study27 in Nature Communications, which found no viable virus in PCR-positive cases at all. The study evaluated data from 9,865,404 residents of Wuhan, China, who had undergone PCR testing between May 14 and June 1, 2020.
A total of 300 tested positive but had no symptoms. Of the 34,424 people with a history of COVID-19, 107 tested positive a second time. Yet, when they did virus cultures on these 407 individuals who had tested positive (either for the first or second time), no live virus was found in any of them!
Antibody Tests Are Equally Unreliable
Antibody tests are also turning out to have their share of quality problems. If you have antibodies against SARS-CoV-2, that would be evidence that your immune system successfully overcame the virus at some point in the past. However, the COVID-19 antibody test may also turn out positive if you have antibodies against common cold viruses.
June 30, 2020, the CDC admitted that prior exposure to coronaviruses responsible for the common cold can result in a positive COVID-19 antibody test, even if you’ve never been exposed to SARS-CoV-2 specifically.28
The saving grace is that studies29,30,31 suggest antibodies produced following exposure to coronaviruses that cause the common cold also appear to provide some general and long-lasting resistance against SARS-CoV-2.
One such study,32,33 published May 14, 2020, in the journal Cell, found 70% of samples from patients who had recovered from mild cases of COVID-19 had resistance to SARS-CoV-2 on the T-cell level, as did 40% to 60% of people who had not been exposed to SARS-CoV-2.
According to the authors, this suggests there’s “cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.” In other words, if you’ve recovered from a common cold caused by a particular coronavirus, your humoral immune system may activate when you encounter SARS-CoV-2, thus rendering you resistant to COVID-19.
Another study34 discovered SARS-CoV-2-specific antibodies are only found in the most severe cases — about 1 in 5. So, a negative antibody test doesn’t necessarily rule out the possibility that you’ve been infected and didn’t get sick. In fact, this finding suggests COVID-19 may actually be five times more prevalent than suspected — and five times less deadly than predicted.
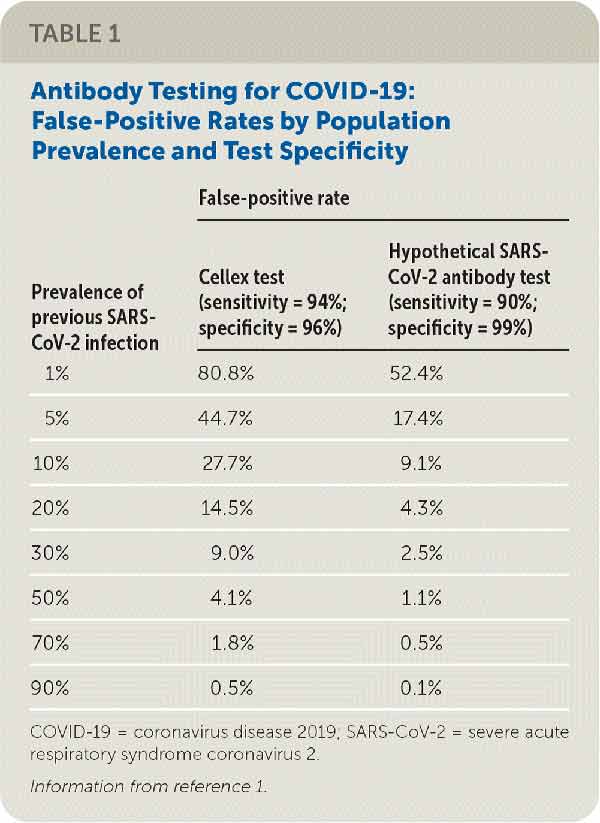
In a letter to the editor35 published in the July 1, 2020, issue of American Family Physician, Drs. Mark Ebell, deputy editor for evidence-based medicine for the journal, and Henry Barry, reviewed some of the available data, noting that:
“When assessing whether patients had a previous infection and may be immune, it is important to avoid false-positives so that patients do not think they are immune when they are not.
Table 1 summarizes the false-positive rates at various population prevalence for the Cellex test and for a hypothetical test that is 90% sensitive and 99% specific. At relatively low population prevalences, which likely reflect current conditions in the United States and elsewhere, we would argue that false-positive rates are unacceptably high with the Cellex test.”
Ebell and Barry pointed out that many of the antibody tests that have provisional approval from the FDA still have not even been evaluated for accuracy. They also recommended that labs report test results “in a way that reflects the local population prevalence based on widespread testing and include the false-positive rate,” as this information “is needed to help family physicians better inform shared decision-making regarding previous infection and return to work or school.”
At present, you’d be hard-pressed to find anyone including that data in their reporting, and the way things are going, I wouldn’t hold my breath in anticipation of such helpful numbers being included in the future either.
High Time to End Mass Testing Scam
If the vast majority of people who test positive for COVID-19 infection have no symptoms, don’t feel sick and don’t look sick, is COVID-19 really a “deadly” disease? Or, is it more like HPV — a viral infection that most people have without knowing it, and which 90% are able to eliminate without treatment?
The primary justification for the tyrannical governmental interventions of COVID-19 was to slow the spread of the infection so that hospital resources would not be overwhelmed, causing people to die due to lack of medical care.
These interventions were not about stopping the spread altogether or even reducing the number of people that would eventually get infected. They certainly were never meant to prevent all death. Any rational analysis would rapidly conclude that this simply isn’t possible, under any circumstance.
Short-term stay-at-home orders and business closings were only intended to slow down the spread so that, eventually, naturally-acquired herd immunity — the best kind — would prevent it from reemerging. Yet the goal posts keep shifting as we go along.
Two-week lockdowns turned into months in some areas. Eventually, we were told everything would go back to normal as soon as a vaccine became available. But once the vaccines started rolling out, the narrative changed again, and we were told we’d still need masks, social distancing and lockdowns well into 2021 or even 2022 even with a vaccine. What, exactly, is going on?
The only rational reason for why government interventions continue is because they’re meant to erode our personal freedoms and civil liberties and transfer wealth to unelected technocrats who are controlling the pandemic narrative. It’s all fearmongering based on a combination of wildly manipulated data and flawed tests.
Aside from PCR testing data, there’s no evidence of a lethal pandemic at all. As mentioned, while there is such a thing as COVID-19, and people have and do die from it, there are no excess deaths due to it.36,37,38 The total mortality for 2020 is normal.
So, unless we think we should shut down the world and stop living because people die from heart disease, diabetes, cancer, the flu or anything else, then there’s no reason to shut down the world because some people happen to die from COVID-19.
What You Can Do
The good news is the hoax is starting to be exposed. In November 2020, a Portuguese appeals court ruled39,40 that the PCR test is “not a reliable test for SARS-CoV-2” and that “a single positive PCR test cannot be used as an effective diagnosis of infection.” Therefore, “any enforced quarantine based on the results is unlawful.”41 The court also noted that forcing healthy people to self-isolate could be a violation of their fundamental right to liberty.
As detailed in “Coronavirus Fraud Scandal — The Biggest Fight Has Just Begun” and “German Lawyers Initiate Class-Action Coronavirus Litigation,” additional legal cases are also to be expected, all of which will help expose the fraud perpetrated. As for what you can do in the meantime, consider:
Turning off mainstream media news and turning to independent experts — do the research. Read through the science.
Continue to counter the censorship by asking questions — arm yourself with mortality statistics and the facts on PCR testing, so you can explain how and why this pandemic simply isn’t a pandemic anymore.
If you are a medical professional, especially if you’re a member of a professional society, write an open letter to your government, urging them to speak to and heed recommendations from independent experts.
Sign The Great Barrington Declaration,42 which calls for an end to lockdowns.
Join a group so that you can have support — Examples of groups formed to fight against government overreach include Us for Them, a group campaigning for reopening schools and protecting children’s rights in the U.K., and the Freedom to Breathe Agency, a U.S. team of attorneys, doctors, business owners and parents who are fighting to protect freedom and liberty.
No comments:
Post a Comment