There is good reason to argue that we are seeing carefully selected switching out of events to reflect a chosen narritive aimed at launcing the global immunization drive by Bil Gates et al. If true, then it all was fraud. It is thus likely that the whole China tale was also part of the scheme.
That is what the evidence really supports. Recall that a recount in italy collapsed 80% of the death causes. It all still boils down to death by flu or common cold.
Evidence of fraud keeps boiling up everywhere and the disease profile is clearly arrested by strong doses of Vitamin C and the quinine derived med. Vitamin D and zinc help out as well for those lacking sun.
According To CDC Data, It’s NOT COVID-19 Coronavirus That Is Causing All The Severe Lung Deaths
By Bill Sardi
April 24, 2020
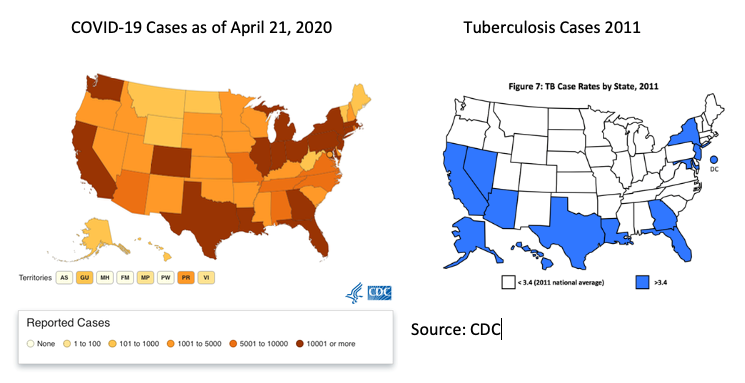
Examine the maps below. They show the States where COVID-19 cases occur which correlates with where tuberculosis of the lungs is prevalent. Either of two conclusions can be made from these maps:
1) Either people living in these States have weak immunity and therefore are likely to develop COVID-19 coronavirus or tuberculosis, or both; and/or
2) The fact most cases of lung pathology occur along the southern border and New York City, where immigrants enter the country, typically with dormant or latent cases of TB. TB may be an uninvestigated co-morbidity that is causing many deaths attributed to COVID-19 coronavirus.
In the next graphic (below) the top chart indicates mortality from pneumonia and influenza only for 2016-2020 with a dramatic up-spike (red line) in early 2020. The bottom chart displays data for total deaths from COVID-19 coronavirus in addition to pneumonia and influenza for Oct. 2015-April 2020 with a sharp increase in the third and fourth months of 2020 (red line). When both charts are compared, it is obvious that the reported increase in deaths is largely due to pneumonia or influenza, not COVID-19.

The next chart compares deaths from COVID-19 coronavirus, deaths due to pneumonia and deaths due to influenza.
By the 11th week of the 2020 pandemic (late March), COVID-19 deaths comprised just 0.1% (one tenth of one percent). This was because the CDC issued test kits that were contaminated with COVID-19 that were withdrawn, resulting in delays in estimating the infectiousness of this coronavirus, and hindered others from producing test kits while the FDA withheld imported tests over quality-control issues. This is how the COVID-19 coronavirus spread in what appears to be an orchestrated effort to let it get out of hand.
A week later COVID-19 (week 12 in the 2020 flu season) as a percentage of deaths in the U.S. were 0.9%, then 4.0% a week later and finally 6.9% by the 14th week (mid-April). These death numbers provided by the CDC are 80% exaggerated because we later find 8 in 10 deaths involved co-morbidities (cancer, diabetes, heart disease) which were the true causes of death. In these patients, it is likely they died with but not of COVID-19.
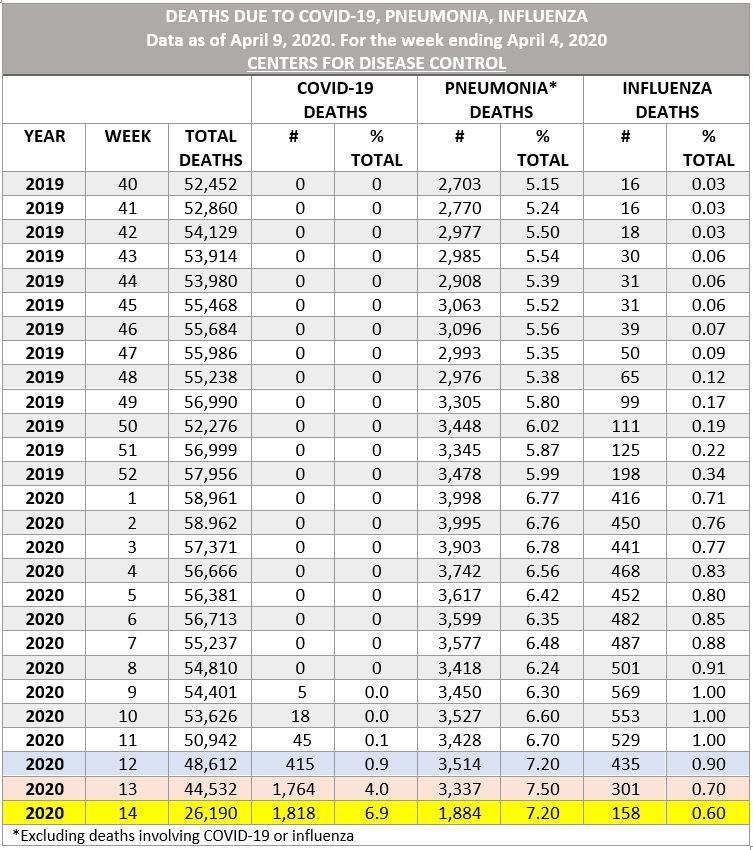
In weeks 12-14 (March-April) of 2020 we see a huge drop off of pneumonia-related deaths from 3,337 to 1,884 and influenza-related deaths from 435, then 301 and finally 158 deaths into the first week of April 2020. The sudden explosion of COVID-19 deaths to 1818 in the 14th week of the flu season appears to be a result of taking death numbers away from pneumonia and influenza and re-classifying them as COVID-19.
Pneumonia deaths declined by 1640 and flu deaths by 277 for a total of 1,917 and deaths attributed to COVID-19 suspiciously rose by 1,403 over a 2-week period.
The CDC almost admits this. Here is their language. According to the CDC, in very small print, “the number of hospitalizations (for influenza) estimated so far this season is lower than end-of-season total hospitalization estimates for any season since CDC began making these estimates.” Suddenly more people were getting COVID-19 and not the flu.
Also look at the dramatic decline in overall deaths in week 14 from 44,532 the prior week to just 26,190. Nothing is said about this. The advocates of quarantine are likely to take credit for this. But it is more likely this striking decline in overall mortality emanates from doctors and hospitals forgoing elective surgery and almost closing down altogether because healthcare personnel fear the dreaded COVID-19. Historically, doctor strikes result in a steep decline in mortality. One such doctors strike in Israel in 1983 has been widely reported. During that 1-month strike funeral directors reported deaths declined from 153 in May of 1999 to 93 deaths in May of 2000 (a 60% decline).
One of the reasons for mis-coding pneumonia cases to COVID-19 cases may be the financial incentives offered to hospitals and doctors to do so. Why did the CDC issue billing coding for hospitals to follow for COVID-19 cases which literally bribed doctors and hospitals to up-code normal pneumonia cases to COVID-19 cases which were reimbursed at a 3-fold higher rate (13,000 to $39,000); normally Medicare would issue such a directive, not the CDC.
The next chart shows that the number of laboratory-confirmed flu hospitalizations began to rise in late 2019 and started to flatten in early March of 2020. So, according to the chart below, presumably it must have been influenza that drove the reported increase in hospitalizations and deaths in mid-March into April 2020. But given that death rates for the flu are widely overstated by the CDC, even that presumption must be rejected. What we are left with is are the ~50,000 cases of pneumonia, which largely occur among elderly adults, that have been mis-coded into COVID-19 deaths.

According to the CDC a total of 19,845 laboratory-confirmed influenza-associated hospitalizations were reported by FluSurv-NET sites between October 1, 2019 and April 11, 2020 with a cumulative hospitalization rate of 68.3 per 100,000 population.
According to CDC published data, 7,071 hospitalized influenza patients have died so far this flu season. That would represent a horrific 35.6% death rate for patients hospitalized for the flu, which must be some kind of giant error (7,071 deaths among 19,845 lab-confirmed hospitalizations).
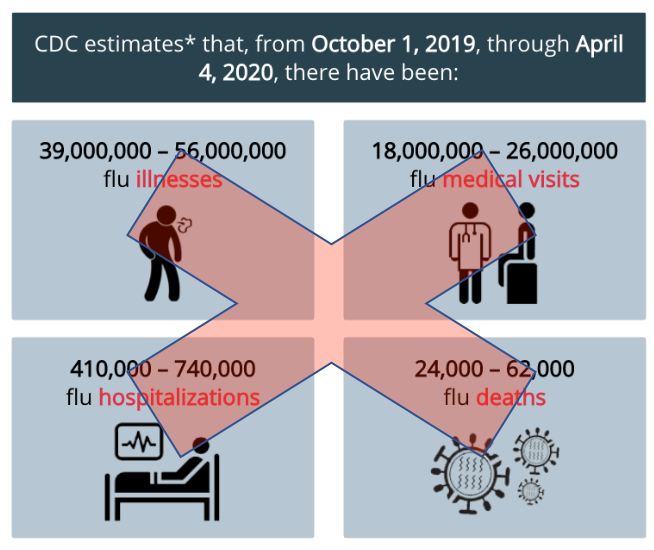
And 7,071 flu-related deaths wouldn’t even be close to the estimates the CDC issued elsewhere for the period of October 1, 2019 through April 4, 2020 (24,000 to 62,000 flu deaths) or the disputed flu-death numbers it issues in its press releases (36,000). In 2018 the CDC said 80,000 people died of the flu in the U.S. Pick a number: 7,071, 24,000, 62,000, 36,000, 80,000.
Fighting an infodemic
While the WHO website claims “We’re not just fighting an epidemic, we’re fighting an infodemic,” and “WHO continues to provide timely and accurate information, in a world where we have an overabundance of information, some accurate, some not,” the WHO and the CDC are the largest source of misinformation regarding seasonal flu, coronavirus and tuberculosis.
Every flu season the CDC rolls out its frightening claim 36,000 Americans die of the flu in order to frighten the public to vaccinate. An alternate source, the American Lung Association, reveals in some years the flu only resulted in a few hundred deaths, with pneumonia and tuberculosis being primary causes of lung-related mortality.
The CDC combines flu deaths with deaths from pneumonia. But according to the American Lung Association, when pneumonia deaths are removed, no more than 3550 Americans died of the flu in any years for the period 1999-2013. During that 15-year period, an average of 1312 Americans died of the flu annually.
While far more people die of tuberculosis (which is what many of the reported COVID-19 deaths are more likely to be caused by), a mutated coronavirus that is highly infectious is only highly mortal in the minds of politicians, public health authorities and those that would profit off of the development of vaccines.
How many infected?
Public health authorities may have to walk back on their preliminary estimates that ~50% of the public has been infected with coronavirus. A recent population study, conducted in Santa Clara County, California, reveals the number of reported COVID-19 cases may be 50-85-times higher than previously estimated. COVID-19 antibodies were found in only 2.49-4.16% of the population. Therefore, the death rate is no worse than the over-stated flu death numbers, if you can make sense of that. Maybe 0.3% die of COVID-19 by loose definition it caused rather than was only associated with a mortal outcome.
What are COVID-19 deaths attributed to?
Worldometer reports as of April 14, 2020, 75.3% of COVID-19 deaths were due to underlying conditions (5151 of 6839) in New York City.
The seasonal onset of the disease is best explained as an onset of a viral disease due to a deficiency of sunshine vitamin D rather than an unexplained eruption of a coronavirus out of nowhere. It has not been proven that COVID-19 coronavirus is a cause of severe lung congestion. In fact, it may be a standby virus. To repeat, many people die with but not of coronavirus. No evidence has been presented so far that COVID-19 is causal in any deaths, or now, COVID-19.
It is inexplicable to see such drastic measures taken for a virally-induced infection that is far less deadly than seasonal tuberculosis, a lung disease that largely affects foreign-born immigrants in the U.S.
The fear-based WHO/CDC/Bill Gates “predictive contagion model” that forecast millions of deaths has been replaced with real data. But it was that “predictive contagion model” that influenced politicians to lockdown and quarantine the public.
The irony of this epidemic and its mandated lockdown of human populations has resulted in irreversible loss of income and destruction of wealth, enough to cut the standard of living in the United States in half, yet ironically there may never be a coronavirus vaccine.
If there is no future vaccine, and no approved medicine, this means the public is left to fend for themselves without medical direction. Why even listen to public health authorities whose numbers simply can’t be relied upon. The news media is irresponsible for buying into the fabricated numbers the CDC issues every year.
That the CDC over-states annual flu deaths in order to scare the public into getting flu shots is one thing, but to frighten the public into a lockdown that destroys family wealth, un-employs millions, increases disease to the extent indoor living results in a decline in vitamin D levels, is something else.
Telling report: maybe it never was the flu virus
A telling study of the misdirection of flu vaccination is revealed in a study of elderly nursing home patients, published in the journal Epidemiology & Infection in 1990. While flu vaccination ranged from 15-90% in nursing homes, the prevalent respiratory infections were not flu viruses but rather cold viruses such as respiratory syncytial virus and coronaviruses. In humans, coronaviruses cause 10-35% of colds. It is noted that reinfection with coronaviruses is common with infectious outbreaks typically during winter and early spring when influenza is prevalent. So, coronavirus outbreaks are old news.
The false presumption is many respiratory tract infections are due to influenza. Given there are studies showing flu shots to be effective at reducing mortality regardless of the predominant flu virus strain in circulation and the common mismatch of the virus in the vaccine, this would suggest any exposure to a pathogenic agent as delivered by needle injection may activate the immune system to produce antibodies. That is how probiotics like Acidophilus work, by introducing non-pathogenic bacteria into the digestive tract to provoke an immune response.
Conclusion: What can be concluded from a pile of misinformation distributed by the CDC? Based upon current data issued by the CDC, it is likely the reported COVID-19 deaths emanate from re-classifying pneumonia deaths to COVID-19 deaths. Pneumonia largely occurs among the elderly. When lung syndrome deaths occur in younger-aged adults, that is probably tuberculosis, which isn’t even on the scoreboard despite being widespread, highly prevalent and potentially deadly.
Copyright © Bill Sardi, writing from La Verne, California. This article has been written exclusively for www.LewRockwell.com and other parties who wish to refer to it should link rather than post at other URLs.
No comments:
Post a Comment