
You understand that politicians were bribed to push this vracket, particularly in India were such behavior is blatent and endemic.
The numbers are actually horrific and may well inspire a serious political backlash.
Now it gets worse as later numbers began to come in. How bad can it be? This all about the jab and since we have maxed out the cdelivery, they have stopped spending on the BS propaganda. Now we really get the science. Recall noone knew about 6,000,000 jews until the war was over, and had they ended the kill program four months earlier, we would still be discovering the truth.
this is were we can get real numbers. What else has been hidden ?
Bombshell. India’s “Shock” and Sudden Excess Mortality (April-July 2021), Caused by Covid Vaccine Rollout In its Early Stages?
Global Research, December 07, 2022
Region: Asia
Theme: Science and Medicine
All Global Research articles can be read in 51 languages by activating the Translate Website button below the author’s name.
To receive Global Research’s Daily Newsletter (selected articles), click here.
Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
***
Abstract
India experienced a unique, sudden, unprecedented and extraordinarily large excess all-cause mortality event in April-July 2021, which is not adequately explained as a “second wave” or as being caused by a new variant of concern. After an overview of four recently published studies that have quantified the April-July 2021 excess all-cause mortality event, we give ten numbered arguments as to why we conclude that the extraordinary mortality event was caused by India’s vaccine rollout in its early stages. Therefore, it appears that the early rollout of the vaccine in India in April-July 2021 was devastating, causing the deaths of approximately 3.7 million residents, on administering approximately 350 million doses of the vaccine.
*
India experienced an extraordinary excess-mortality shock in April through July 2021, not seen in any other country in the world.
The mortality by week rose to almost 700% of its baseline value in April 2021, based on 90 municipalities in the state of Gujarat (Acosta et al. 2022; their Fig. 2), and the mortality by month rose to almost 400% of its baseline value in July 2021, based on 19 Indian states, 1.27 billion population (Leffler et al. 2022; their Fig. 1). To be clear, this represents all-cause mortalities that are 7-fold (by week) and 4-fold (by month) greater, respectively, than the pre-Covid (2019) all-cause mortalities in India.
This 4-month April-July 2021 excess mortality event in India is described in four independent studies published in leading medical journals (Acosta et al. 2022; Jha et al. 2022; Leffler et al. 2022; Lewnard et al. 2022); and it represents the great majority of excess all-cause deaths for the entire Covid period examined since a pandemic was declared by the World Health Organization on 11 March 2020.
Given the extraordinary characteristics of the 4-month April-July 2021 excess mortality event in India, it is useful to reproduce key figures from the said studies, in order to grasp its significance and nature, as follows.
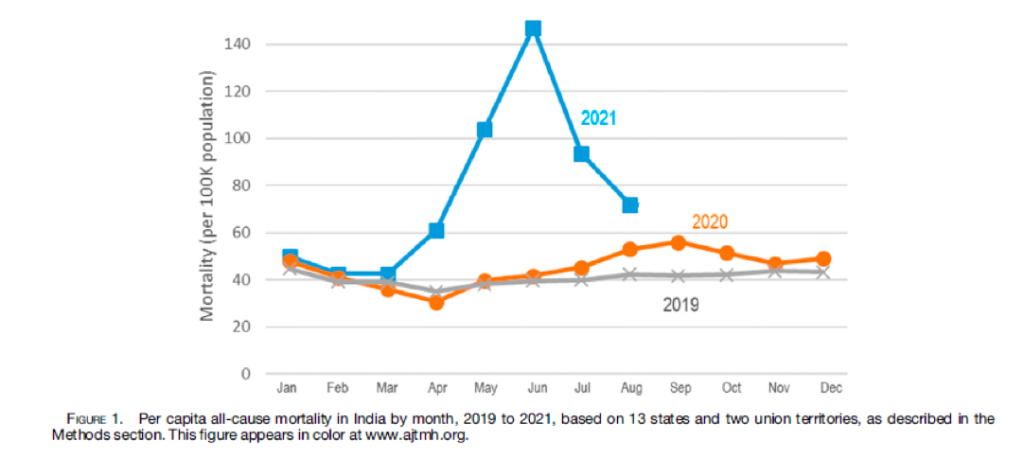
Figure 1: Leffler et al. (2022), using 19 Indian states, 1.27 billion population, their Fig. 1.
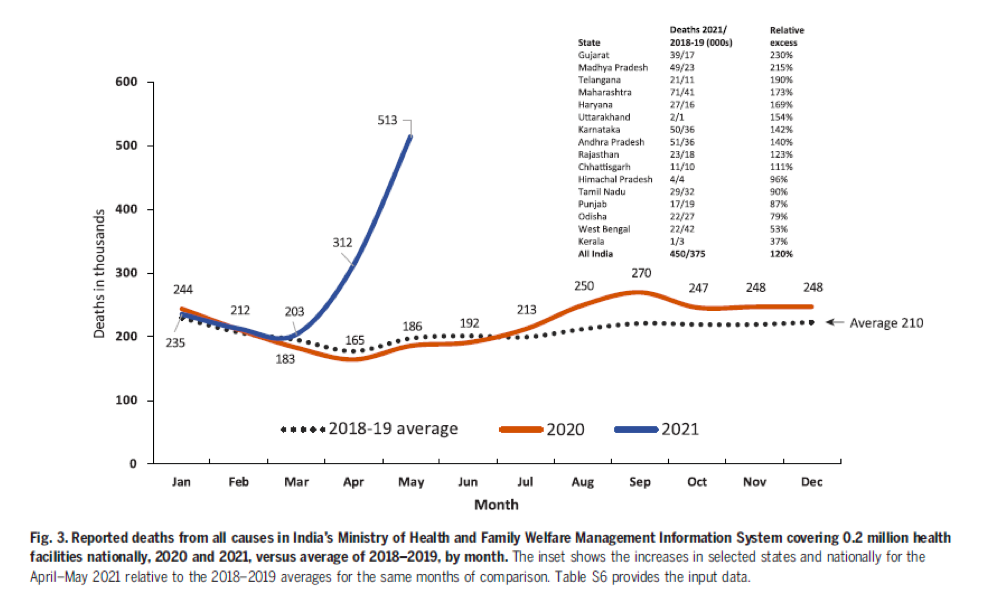
Figure 2: Jha et al. (2022), using 0.2 million health facilities nationally, their Fig. 3. This is essentially the same figure as Fig. 1 in Deshmukh et al. (2021).
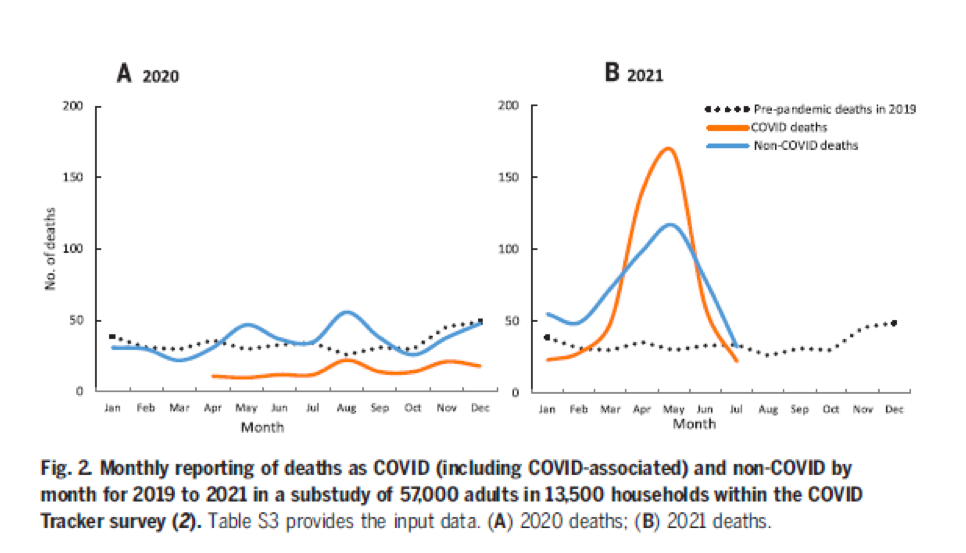
Figure 3: Jha et al. (2022), using a survey study of 57 thousand adults, their Fig. 2.
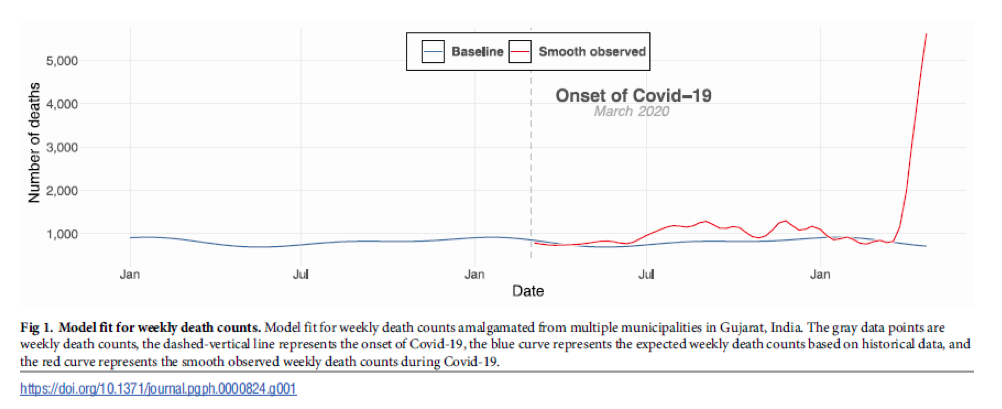
Figure 4: Acosta et al. (2022), using death certificates from 90 municipalities in the Indian state of Gujarat, their Fig. 1.
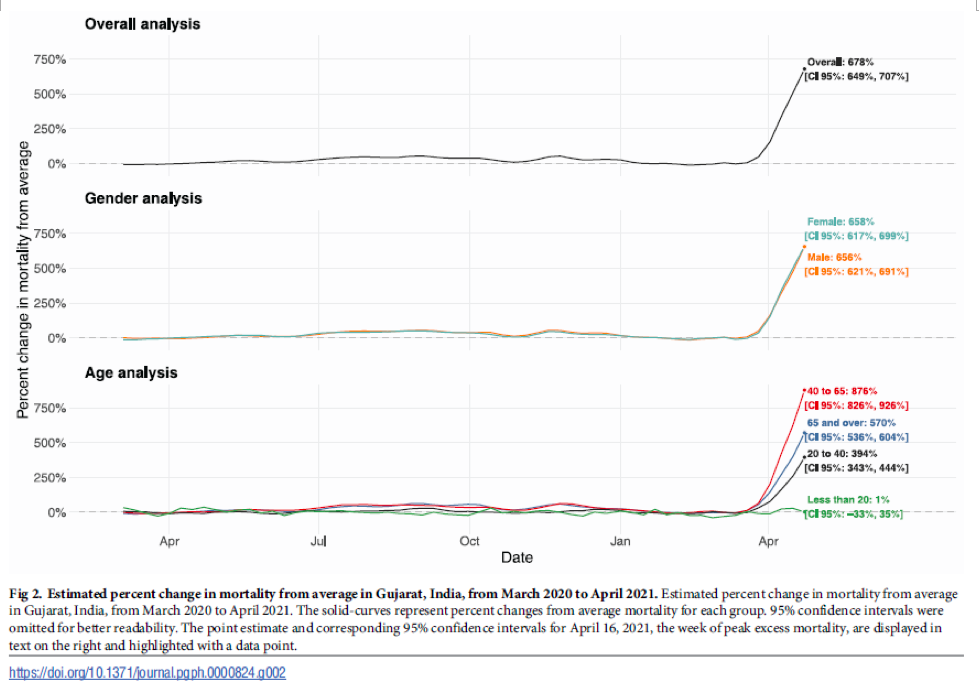
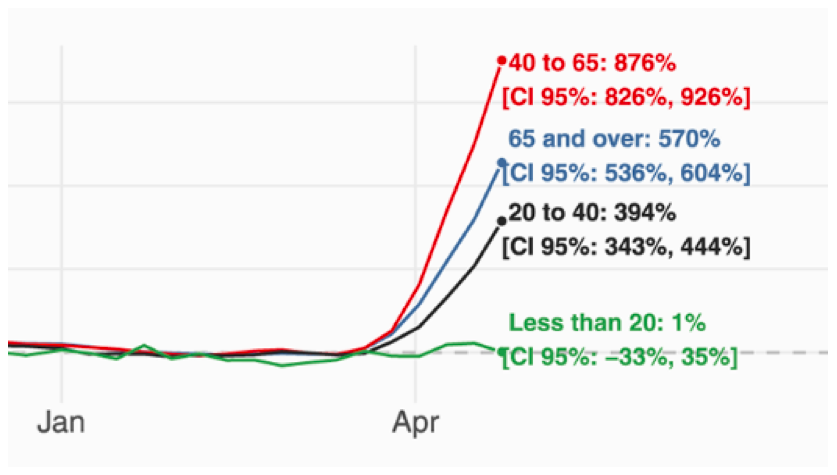
Figure 5: Acosta et al. (2022), using death certificates from 90 municipalities in the Indian state of Gujarat, their Fig. 2. Based on mortality by week. (Upper) Full figure. (Lower) Selected enlargement.
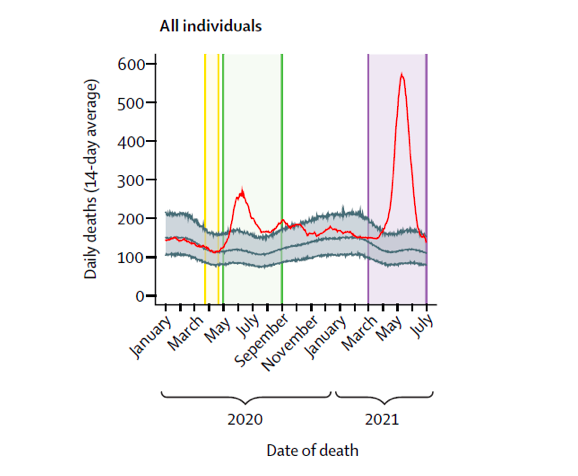
Figure 6: Lewnard et al. (2022), in the Chennai district, India, their Fig. 1. (Red line: 14-day moving average estimates of daily mortality in 2020 and 2021 (observed deaths), corrected for lagged reporting based on 2019 observations.)
When such a large, unique, and sudden feature in mortality of all causes occurs in any jurisdiction, it demands thorough investigation, if the cause is not empirically obvious, such as a massive earthquake or a genocidal military attack. This holds even during a declared pandemic, given the unique, sudden, unprecedented and large-magnitude nature of the event in India.
All of the above-cited authors who have reported on the 4-month April-July 2021 excess mortality event in India have referred to the event as being India’s “second wave” and have used their all-cause mortality evaluations to infer that COVID-19 mortality is potentially largely underestimated by India’s official Covid-death statistics.
In this author’s opinion, if that was India’s “second wave” then, by comparison, India virtually did not have a “first wave”, and essentially did not have a death-causing pandemic prior to April 2021.
None of the above-cited authors who have reported on the 4-month April-July 2021 excess mortality event in India have mentioned the remarkable coincidence that the said excess mortality event coincides in time with India’s vaccine rollout, starting on 1 March 2021 with those 60 years and older and those over 45 years and having “comorbidities” (among 20 listed comorbidities) (The Economic Times, 24 February 2021; Ministry of Health and Family Welfare, Government of India, 2021), extended to all residents over 45 years on 1 April 2021; and coinciding in time with the government’s 4-day Teeka Utsav (“Vaccine Festival”) from 11 to 14 April 2021, in which some 100 million vaccine doses were administered by its completion: “Elderly people or those who may not be much educated should be helped in getting the vaccine”, Prime Minister Modi said (Mint, 11 April 2021).
To appreciate India’s vaccine rollout, its official statistics are a reference, as follows.
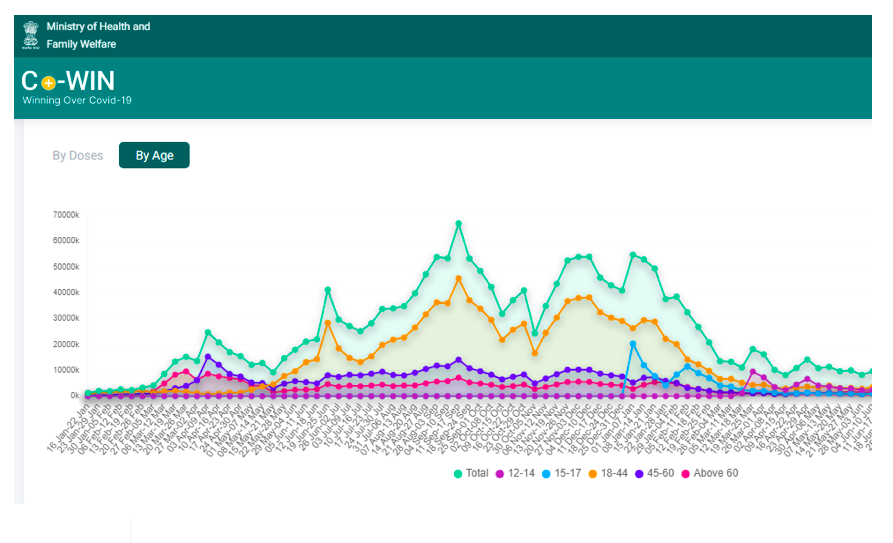
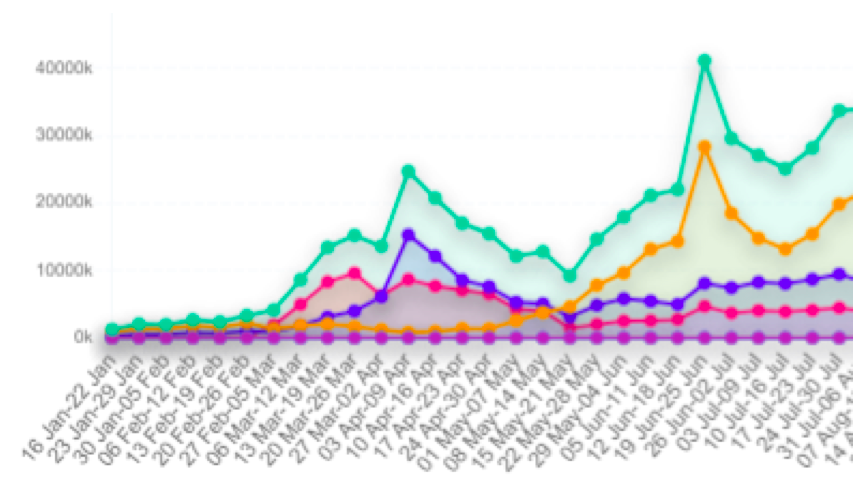
Figure 7: Ministry of Health and Family Welfare, Government of India (2022): C+ WIN dashboard, by age as indicated. (Upper) Broad view. (Lower) Selected enlargement.
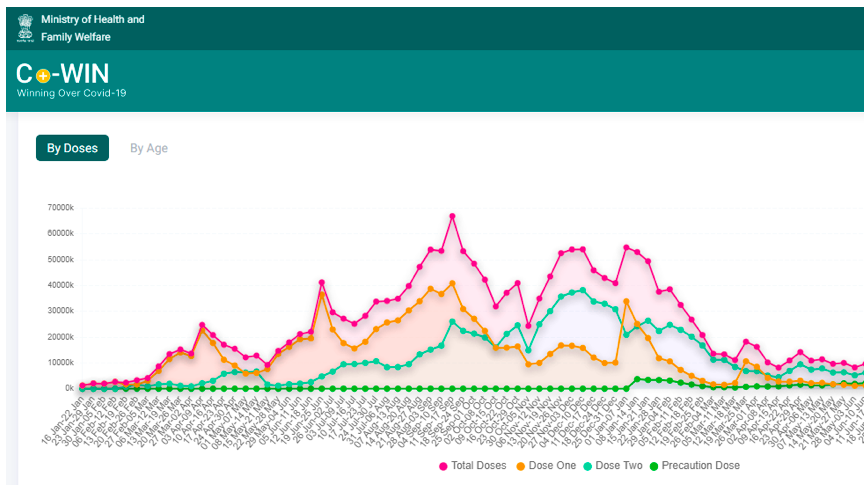
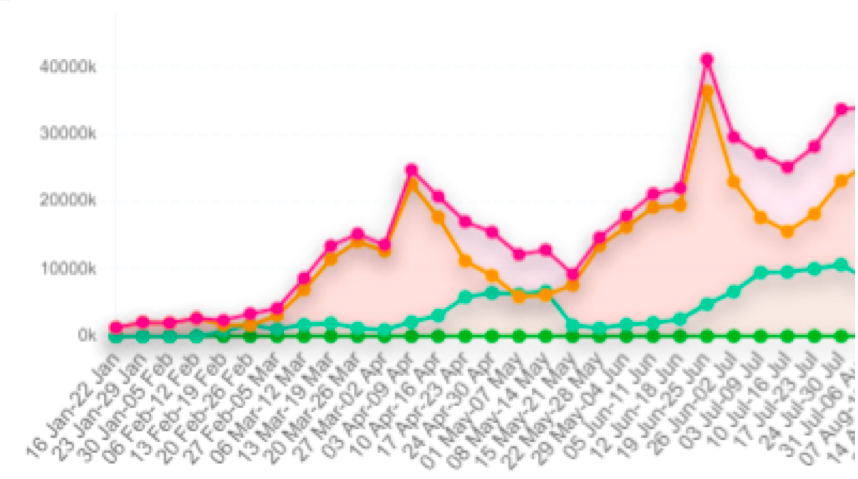
Figure 8: Ministry of Health and Family Welfare, Government of India (2022): C+ WIN dashboard, by dose type as indicated. (Upper) Broad view. (Lower) Selected enlargement.
For the following reasons (presented as numbered points), taken together, we conclude that the 4-month April-July 2021 surge in excess all-cause mortality in India may largely or predominantly have been caused by the vaccine rollout in its early stages.
1. The mortality event is unique to India, sudden, unprecedented, massive and synchronous with India’s vaccine rollout to the most elderly and most fragile (comorbidity) residents (Figures 1-8).
2. By comparison, in relative terms, there were no significant mortality events and there was no significant cumulative excess mortality prior to April 2021, during more than a year of the declared pandemic (Figures 1-6).
The declared pandemic would have had to spare India for more than a year, while it raged in many other places around the world, before it showed a dramatic many-fold increase in virulence, suddenly in April-July 2021, when vaccines coincidentally were being rolled out to the elderly and those having comorbidities.
3. The early rollout of the vaccine was not executed following the original ambitious plan but instead was at first delayed by implementation difficulties and then boosted by an ad hoc government intervention (Prime Minister Modi’s 11-14 April 2021 Teeka Utsav, “Vaccine Festival”), which encouraged accelerated blanket and penetrating delivery to the poor, uneducated, and those presumed to be most in need.
4. A similar synchronicity between increased vaccination associated with a government intervention to accelerate vaccine delivery and an anomalous surge (peak) in all-cause mortality is observed in connection with the so-called “vaccine equity” campaigns in the USA. An anomalous fall-2021 peak was interpreted as being caused by the vaccines, and is prominent in the 25-64 years age group in 21 states of the USA, most notably including Alabama, Mississippi, Georgia, Florida and Louisiana (Rancourt et al., 2022). The data for Mississippi is shown below (Figure 9).
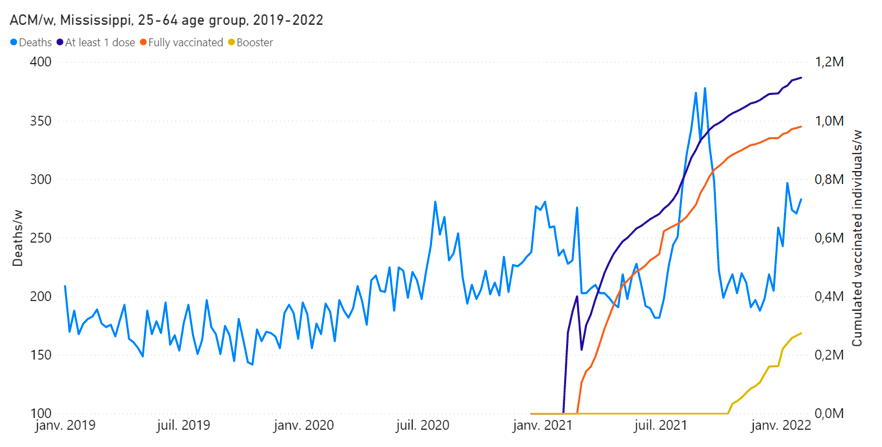
Figure 9: Rancourt et al. (2022), their Fig. 11B. All-cause mortality by week (light-blue), cumulated number of people with at least one dose of vaccine (dark-blue), cumulated number of fully vaccinated people (orange) and cumulated number of people with a booster dose (yellow) by week from 2019 to 2022, for 25-64 years age group in Mississippi. Data are displayed from week-1 of 2019 to week-5 of 2022.
In the study by Rancourt et al. (2022), it was concluded that significant (detectable by all-cause mortality) vaccine-induced mortality occurred primarily among fragile groups, characterized by high degrees of poverty, disability, obesity, diabetes, and high medication rates. The vaccine injection was seen as an additional challenge, often accelerating and causing death in residents with comorbidities.
5. The magnitude of the April-July 2021 excess all-cause mortality event (normalized by population) is highly heterogeneous from region to region in India (above-cited references). This suggests that the net regional excess mortality is related to the underlying heterogeneity of health status, and to differences in health-status group selection, which were actually vaccinated in a region; rather than being due to a given infection fatality ratio (and its age profile) for the rapid spread of an infectious disease, applied to all regions similarly.
6. The April-July 2021 excess all-cause mortality event occurs simultaneously across India, as do the national vaccine rollout and Prime Minister Modi’s “Vaccine Festival” intervention, rather than showing any distribution of starting times, which would be compatible with a spreading infectious disease seeding different regions at different times and spreading at different rates depending on regional differences of social and health conditions.
7. The April-July 2021 excess all-cause mortality, at least initially, is significantly larger, on a mortality-baseline-percent basis for mortality by week, for 40-64 year old residents than for 65+ year old residents (~880% vs ~570%) (Figure 5). This is incompatible with controlled clinical studies and empirical observations, which find that infection fatality probability of COVID-19-assigned death is exponential with age (Bonanad et al., 2020; Goldstein and Lee, 2020; Santesmasses et al., 2020; Bauer et al., 2021; Elo et al., 2022; Sorensen et al., 2022). However, the age-dependence behaviour is similar to what is observed for the vaccination period of the Covid period compared to the pre-vaccination Covid period in the USA (Rancourt et al., 2022; see their Fig. 17).
8. The Vaccine Adverse Event Reporting System (VAERS) of the USA unambiguously shows excess all-cause deaths immediately following injections with each of the three types of COVID-19 vaccines used in the USA, with a prominent peak within 5 days of injection and an exponentially decaying excess mortality extending 2 months following injection (Hickey and Rancourt, 2022; see their Figs. S3 through S5). The integrated mortality by number of injections following injection (injection toxicity) increases exponentially with age, as does the batch to batch variability of toxicity (Hickey and Rancourt, 2022; see their Fig. S6). The latter observations of exponential increases with age mean that the injections represent fatal challenges in proportion to frailty of the subject.
9. Detailed histopathological and immunohistochemical autopsy studies have demonstrated that the COVID-19 vaccines are causes of death, both in otherwise healthy subjects and in elderly subjects with comorbidities (Choi et al., 2021; Schneider et al., 2021; Sessa et al., 2021; Gill et al., 2022; Mörz, 2022; Schwab et al., 2022).
10. We have not found any study establishing that there was a sudden rise (and fall) of any disproportionately virulent variant of concern that would have been synchronous with or swept through and caused the April-July 2021 excess all-cause mortality event. For example, Dhar et al. (2021) postulate that the April-July 2021 “second wave” event in Delhi (the capital city of India) was due to the Delta variant, which would have quickly swept Delhi to become predominant because it would have higher transmissibility and larger immune escape than concomitantly circulating variants. However, Dhar et al. estimate the needed characteristics of Delta by fitting a model to the epidemiological data and to the variant predominance estimated by genomic measurements from small non-randomized cohorts. Leaving aside the large known and unknown uncertainties throughout their exercise, basically, the inferred characteristics of Delta are obtained by fitting to the data, rather than being independently measured in a controlled clinical trial. Under such circumstances, the mortality event creates an illusion of the needed Delta, but an actual Delta cannot be concluded to have caused the mortality event.
In conclusion, it appears that the early rollout of the vaccine in April-July 2021 in India was devastating, causing the deaths of approximately 3.7 million residents (Figure 1), on administering approximately 350 million doses of the vaccine (in a population of 1.39 billion).
This corresponds to an effective vaccine fatality per dose ratio (per-dose toxicity) of approximately 1%, which is approximately x100 the vaccine fatality per dose ratio for the Janssen vaccine administered to 65+ year old residents of the USA, calculated from the VAERS data (Hickey and Rancourt, 2021; see their Table 1). It is also approximately the same vaccine fatality per dose ratio (1%) as is consistent with the anomalous fall-2021 peak in excess all-cause mortality occurring in high-poverty states of the USA, which was interpreted as being caused by the vaccine: Rancourt et al. (2022) and see the data for Mississippi shown in Figure 9.
Frail residents are susceptible to being fatally harmed on injection and should be protected against overly enthusiastic or politically motivated state-run injection campaigns implemented without stringent individual clinical risk assessment.
*
Note to readers: Please click the share buttons above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Denis G. Rancourt, PhD is a Researcher at Ontario Civil Liberties Association (ocla.ca).
Sources
Acosta et al. (2022): Acosta RJ, Patnaik B, Buckee C, Kiang MV, Irizarry RA, Balsari S, et al. /// All-cause excess mortality across 90 municipalities in Gujarat, India, during the COVID-19 pandemic (March 2020-April 2021). /// PLOS Glob Public Health, 2022, 2(8): e0000824. https://doi.org/10.1371/journal.pgph.0000824
Bauer et al. (2021): Bauer, P., Brugger, J., König, F. et al. /// An international comparison of age and sex dependency of COVID-19 deaths in 2020: a descriptive analysis. /// Sci Rep 11, 19143 (2021). https://doi.org/10.1038/s41598-021-97711-8
Bonanad et al. (2020): Bonanad C, García-Blas S, Tarazona-Santabalbina F, Sanchis J, Bertomeu-González V, Fácila L, Ariza A, Núñez J, Cordero A. /// The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis With 611,583 Subjects. /// J Am Med Dir Assoc. 2020 Jul;21(7):915-918. doi: 10.1016/j.jamda.2020.05.045. Epub 2020 May 25. PMID: 32674819; PMCID: PMC7247470. https://doi.org/10.1016/j.jamda.2020.05.045
Choi et al. (2021): Sangjoon Choi, SangHan Lee, Jeong-Wook Seo, Min-ju Kim, Yo Han Jeon, Ji Hyun Park, Jong Kyu Lee, Nam Seok Yeo /// Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings /// Journal of Korean Medical Science 2021; 36(40): e286. DOI: https://doi.org/10.3346/jkms.2021.36.e286
Deshmukh et al. (2021): Yashwant Deshmukh, Wilson Suraweera, Chinmay Tumbe, Aditi Bhowmick, Sankalp Sharma, Paul Novosad, Sze Hang Fu, Leslie Newcombe, Hellen Gelband, Patrick Brown, Prabhat Jha /// Excess mortality in India from July 2020 to July 2021 during the COVID pandemic: death registration, health facility deaths, and survey data /// medRxiv 2021.07.20.21260872; doi: https://doi.org/10.1101/2021.07.20.21260872
Dhar et al. (2021): Dhar MS, Marwal R, Vs R, Ponnusamy K, Jolly B, Bhoyar RC, Sardana V, Naushin S, Rophina M, Mellan TA, Mishra S, Whittaker C, Fatihi S, Datta M, Singh P, Sharma U, Ujjainiya R, Bhatheja N, Divakar MK, Singh MK, Imran M, Senthivel V, Maurya R, Jha N, Mehta P, A V, Sharma P, Vr A, Chaudhary U, Soni N, Thukral L, Flaxman S, Bhatt S, Pandey R, Dash D, Faruq M, Lall H, Gogia H, Madan P, Kulkarni S, Chauhan H, Sengupta S, Kabra S; Indian SARS-CoV-2 Genomics Consortium (INSACOG)‡, Gupta RK, Singh SK, Agrawal A, Rakshit P, Nandicoori V, Tallapaka KB, Sowpati DT, Thangaraj K, Bashyam MD, Dalal A, Sivasubbu S, Scaria V, Parida A, Raghav SK, Prasad P, Sarin A, Mayor S, Ramakrishnan U, Palakodeti D, Seshasayee ASN, Bhat M, Shouche Y, Pillai A, Dikid T, Das S, Maitra A, Chinnaswamy S, Biswas NK, Desai AS, Pattabiraman C, Manjunatha MV, Mani RS, Arunachal Udupi G, Abraham P, Atul PV, Cherian SS. /// Genomic characterization and epidemiology of an emerging SARS-CoV-2 variant in Delhi, India. /// Science. 2021 Nov 19;374(6570):995-999. doi: 10.1126/science.abj9932. Epub 2021 Oct 14. PMID: 34648303; PMCID: PMC7612010. https://doi.org/10.1126/science.abj9932
Elo et al. (2022): Elo, I.T. et al. /// Evaluation of Age Patterns of COVID-19 Mortality by Race and Ethnicity From March 2020 to October 2021 in the US /// JAMA Network Open, 2022, 5(5), p. e2212686. Available at: https://doi.org/10.1001/jamanetworkopen.2022.12686
Gill et al. (2022): James R. Gill, Randy Tashjian, Emily Duncanson /// Autopsy Histopathologic Cardiac Findings in 2 Adolescents Following the Second COVID-19 Vaccine Dose. /// Arch Pathol Lab Med 1 August 2022; 146 (8): 925–929. doi: https://doi.org/10.5858/arpa.2021-0435-SA
Goldstein and Lee (2020): Joshua R. Goldstein, Ronald D. Lee /// Demographic perspectives on the mortality of COVID-19 and other epidemics /// PNAS | August 20, 2020 | 117 (36) 22035-22041 /// https://doi.org/10.1073/pnas.2006392117
Hickey and Rancourt (2022): Hickey, J. and Rancourt, D.G. /// Nature of the toxicity of the COVID-19 vaccines in the USA /// ResearchGate [Preprint] (9 February 2022). Available at: https://www.researchgate.net/publication/358489777_Nature_of_the_toxicity_of_the_COVID-19_vaccines_in_the_USA /// Archived at: https://archive.ph/LZpRj
Jha et al. (2022): Jha P, Deshmukh Y, Tumbe C, Suraweera W, Bhowmick A, Sharma S, Novosad P, Fu SH, Newcombe L, Gelband H, Brown P. /// COVID mortality in India: National survey data and health facility deaths /// Science 375, 667–671, 11 February 2022 /// https://www.science.org/doi/10.1126/science.abm5154
Leffler et al. (2022): Leffler CT, Lykins V JD, Das S, Yang E, Konda S. /// Preliminary Analysis of Excess Mortality in India During the COVID-19 Pandemic. /// The American Journal of Tropical Medicine and Hygiene. 2022;106(5):1507-1510. doi:10.4269/ajtmh.21-0864 . https://doi.org/10.4269/ajtmh.21-0864
Lewnard et al. (2022): Joseph A Lewnard, Ayesha Mahmud, Tejas Narayan, Brian Wahl, T S Selvavinayagam, Chandra Mohan B, Ramanan Laxminarayan /// All-cause mortality during the COVID-19 pandemic in Chennai, India: an observational study /// The Lancet Infectious Diseases, Volume 22, Issue 4, 2022, Pages 463-472, ISSN 1473-3099, https://doi.org/10.1016/S1473-3099(21)00746-5
Ministry of Health and Family Welfare, Government of India (2021): FAQs on COVID-19 Vaccines and Vaccination Program /// https://www.mohfw.gov.in/pdf/FAQsCOVID19vaccinesvaccinationprogramWebsiteupload27Sep.pdf /// accessed on 4 December 2022
Ministry of Health and Family Welfare, Government of India (2022): C+ WIN dashboard, Winning Over COVID-19 /// https://dashboard.cowin.gov.in/ /// accessed on 4 December 2022
Mint (11 April 2021): Staff Writer /// Tika Utsav: PM Modi calls for mass vaccination as India prepares to vaccinate maximum people /// Updated: 11 Apr 2021, 11:24 AM IST /// https://www.livemint.com/news/india/tika-utsav-pm-modi-calls-for-mass-vaccination-as-india-prepares-to-vaccinate-maximum-people-11618118595162.html /// Archived at: https://archive.ph/YPRy2
Mörz (2022): Mörz, M. A /// Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. /// Vaccines 2022, 10, 1651. https://doi.org/10.3390/vaccines10101651
Rancourt et al. (2022): Rancourt, D.G., Baudin, M. and Mercier, J. /// COVID-Period Mass Vaccination Campaign and Public Health Disaster in the USA: From age/state-resolved all-cause mortality by time, age-resolved vaccine delivery by time, and socio-geo-economic data /// Research Gate (2 August 2022) /// https://www.researchgate.net/publication/362427136_COVID-Period_Mass_Vaccination_Campaign_and_Public_Health_Disaster_in_the_USA_From_agestate-resolved_all-cause_mortality_by_time_age-resolved_vaccine_delivery_by_time_and_socio-geo-economic_data /// Also available at: https://vixra.org/abs/2208.0023
Santesmasses et al. (2020): Santesmasses, D., Castro, J.P., Zenin, A.A., Shindyapina, A.V., Gerashchenko, M.V., Zhang, B., Kerepesi, C., Yim, S.H., Fedichev, P.O. and Gladyshev, V.N. /// COVID-19 is an emergent disease of aging. /// Aging Cell, 2020, 19: e13230. /// https://doi.org/10.1111/acel.13230
Schneider et al. (2021): Schneider, J., Sottmann, L., Greinacher, A. et al. /// Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. /// Int J Legal Med 135, 2335–2345 (2021). https://doi.org/10.1007/s00414-021-02706-9
Schwab et al. (2022): Schwab, C., Domke, L.M., Hartmann, L. et al. /// Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. /// Clin Res Cardiol (2022). https://doi.org/10.1007/s00392-022-02129-5
Sessa et al. (2021): Sessa, F.; Salerno, M.; Esposito, M.; Di Nunno, N.; Zamboni, P.; Pomara, C. /// Autopsy Findings and Causality Relationship between Death and COVID‑19 Vaccination: A Systematic Review. /// J. Clin. Med. 2021, 10, 5876. https://doi.org/10.3390/jcm10245876
Sorensen et al. (2022): Sorensen, R.J.D. et al. /// Variation in the COVID-19 infection–fatality ratio by age, time, and geography during the pre-vaccine era: a systematic analysis /// The Lancet, 2022, 399(10334), pp. 1469–1488. /// Available at: https://doi.org/10.1016/S0140-6736(21)02867-1
The Economic Times (24 February 2021): All above 60 years of age, 45-plus with comorbidities can get COVID-19 vaccine from March 1 /// Last Updated: Feb 24, 2021, 06:12 PM IST /// https://economictimes.indiatimes.com/news/politics-and-nation/all-60-citizens-all-45-people-with-comorbidities-to-get-free-covid-shots-at-govt-facilities-from-march-1/articleshow/81189171.cms /// Archived at: https://archive.ph/c2A9D
No comments:
Post a Comment