The science is catching up quickly. Most of the benefirts were deeply suppressed and came out as a surprised. what we are now discovering is non addictive brain medeicines with clear therepeutic benefits.
This work starts the process of providing guidence. It will still require ample clinical practice in order to develop full confidence.
Thjat is slowly starting to happen. Soon enough all will be applying all this. It is noteworthy that the whole opiod industry is in full retreat in the face of the non addictive CBDs and their now clearly superior efficacy.
It is not game over, but it is also soon enough for most of us. Perhaps 'We the People' will take emperical medicine back.
.
Thomas Anderson,
Rotem Petranker,
Adam Christopher,
Daniel Rosenbaum,
Cory Weissman,
Le-Anh Dinh-Williams,
Katrina Hui
Emma Hapke
Abstract
Background
Methods
Results
Conclusions
Introduction
The benefits of full-dose psychedelics
The challenges of full-dose psychedelics
Methods
The present study
Grounded theory method
Respondents
Design and questionnaires
Microdosing benefits and challenges (MDBCs)
Improved health behaviours and reduced consumption
Results
Microdosing substances
Empirical codebook: benefits of microdosing
Categories of benefit
Categories of challenges
Benefits and challenges by microdosing substance
Improvements and reductions
Emergent parallelism
Improvements and reductions
Limitations and future directions
Conclusion
Availability of data and materials
Microdosing
psychedelics is the practice of consuming very low, sub-hallucinogenic
doses of a psychedelic substance, such as lysergic acid diethylamide
(LSD) or psilocybin-containing mushrooms. According to media reports,
microdosing has grown in popularity, yet the scientific literature
contains minimal research on this practice. There has been limited
reporting on adverse events associated with microdosing, and the
experiences of microdosers in community samples have not been
categorized.
In
the present study, we develop a codebook of microdosing benefits and
challenges (MDBC) based on the qualitative reports of a real-world
sample of 278 microdosers.
We
describe novel findings, both in terms of beneficial outcomes, such as
improved mood (26.6%) and focus (14.8%), and in terms of challenging
outcomes, such as physiological discomfort (18.0%) and increased anxiety
(6.7%). We also show parallels between benefits and drawbacks and
discuss the implications of these results. We probe for
substance-dependent differences, finding that psilocybin-only users
report the benefits of microdosing were more important than other users
report.
These
mixed-methods results help summarize and frame the experiences reported
by an active microdosing community as high-potential avenues for future
scientific research. The MDBC taxonomy reported here informs future
research, leveraging participant reports to distil the highest-potential
intervention targets so research funding can be efficiently allocated.
Microdosing research complements the full-dose literature as clinical
treatments are developed and neuropharmacological mechanisms are sought.
This framework aims to inform researchers and clinicians as
experimental microdosing research begins in earnest in the years to
come.
The
practice of microdosing psychedelics involves ingesting
sub-hallucinogenic amounts of a psychedelic substance (e.g. LSD,
psilocybin) and has recently grown in popularity. The number of popular
media accounts and book-length treatments of microdosing has been
growing [1,2,3,4,5,6,7].
Online microdosing communities have grown to the tens of thousands with
more than 40,000 users subscribing to the /r/microdosing subreddit
(/r/microdosing subreddit, Reddit Inc, San Francisco, CA, USA). This
public interest speaks to a social need for scientific studies to inform
the public about the effects of microdosing. Initial scientific
investigations of microdosing are just beginning [8,9,10,11]
(Rosenbaum D, Weissman C, Hapke E, Hui K, Petranker R, Dinh-Williams
L-A, et al.: Microdosing psychedelic substances: demographics,
psychiatric comorbidities, and comorbid substance use, in preparation)
and future directions remain unclear. While full-dose psychedelic
research is growing in prominence and outcomes from full-dose studies
can certainly inform microdosing studies, focusing solely on known
full-dose outcomes could result in missing unanticipated benefits and
challenges specific to microdosing. As such, beginning with an open,
exploratory approach could result in a better understanding of the
potential benefits and challenges specific to microdosing. The present
study aims to provide a data-driven taxonomy describing the positive and
negative experiences reported by microdosers from an open-ended
analysis of microdosing-specific outcomes, summarizing high-potential
avenues for focused experimental investigations.
While more than a thousand early studies linked psychedelic use with beneficial effects [12], there was a 40-year pause on psychedelic research following the prohibition of these substances [13].
Despite continued prohibition, modern research has revealed the
promising potential of LSD and psilocybin for treating alcohol and
tobacco dependence [14,15,16,17], depression [18, 19], and end-of-life anxiety [20,21,22],
while related research on 3,4-methylenedioxymethamphetamine (MDMA) has
shown great promise for treating post-traumatic stress disorder [23]. Psychedelics can also increase openness and occasion mystical-type experiences in healthy controls [24,25,26].
As full-dose psychedelics appear to aide in the relief of severe,
chronic psychiatric conditions (e.g. depression, anxiety, PTSD), milder
mental health concerns may plausibly be treated by lower, recurring
doses. This is especially worth considering if certain full-dose
outcomes are found to rely on purely pharmacologic mechanisms rather
than primarily on phenomenological experiences [27].
Limiting
microdosing research to topics that have been investigated in full-dose
research could prematurely overlook unpredicted and potentially
distinct microdosing outcomes. Full-dose research has employed various
focal assessments of symptomatology, mood, and personality that are
likely applicable to microdosing research, but due to the low doses and
lack of perceptual alteration intended in microdosing, other full-dose
phenomena, such as ego dissolution and mystical-type experiences, are
less relevant to microdosing research. Instead, as a means of preparing
for a broad range of outcomes, the present work solicited open-ended
reports of benefits and challenges. Additionally, as psychedelic
substances act on distinct yet overlapping neural receptor sites, it
seems plausible that distinct patterns could emerge for different
substances. The present study thus included microdosers who used LSD,
psilocybin, or both.
While psychedelics appear to have considerable potential benefits and low physiological risks [28,29,30], full-dose experiences can put participants under considerable psychological risk [31].
In a survey targeting participants that had at least one challenging
experience (“bad trip”) with psilocybin mushrooms, 39% of respondents
rated their full-dose experiences as among the top 5 most
psychologically difficult/challenging experiences of their lives [32]. Griffiths et al. [20]
used both “high” (22 mg/70 kg) and “low” (1 or 3 mg/70 kg) doses of
psilocybin as experimental and control conditions, respectively. A
dose-response effect could be seen such that in the high-dose condition,
32% of participants reported physiological discomfort whereas only 12%
reported the same in the low-dose condition; likewise, 26% reported
anxiety in the high-dose condition versus 15% in the low-dose condition [20]. Delayed-onset headaches are another possible side-effect of full-dose psilocybin [33].
To mitigate these risks, Johnson et al. [31]
proposed safety guidelines for use with full-dose psychedelic
substances, which rely on managing participant inclusion and having a
comfortable, guided clinical setting. As microdosing does not involve
the intensity of experience present in full-dose research, challenging
experiences may be less likely. One may, however, anticipate that less
frequent, less intense versions of full-dose challenges could be present
even at the very low doses used in microdosing (e.g. restlessness
instead of insomnia, mild anxiety instead of fear, mild headaches). As
the study of microdosing is in its infancy, we could also expect there
to be challenges that fall beyond the scope of reports based on full
doses; the present study thus preferred open-ended surveying of
drawbacks over pre-existing focal questionnaires.
In
this study, we explored the benefits and challenges experienced by
microdosers in a cross-sectional, retrospective, anonymous online
survey. Respondents reported their subjective microdosing benefits and
challenges (MDBCs) and the subjective importance of each outcome. We
then used a grounded theory approach [34]
to identify commonly-reported MDBCs and thereby deliver an empirical
MDBC taxonomy to support future microdosing research. We also explored
whether microdosing substances (LSD-only versus psilocybin-only versus
LSD and psilocybin) were associated with different outcomes.
This
study was part of a larger project that reported on the demographic and
psychiatric comorbidities of the sample (Rosenbaum D, Weissman C, Hapke
E, Hui K, Petranker R, Dinh-Williams L-A, et al.: Microdosing
psychedelic substances: demographics, psychiatric comorbidities, and
comorbid substance use, in preparation) as well as a paper that
addressed pre-registered hypotheses concerning mental health,
personality, and creativity variables [8].
Microdosers
were prompted to provide up to three benefits and up to three
challenges associated with microdosing in small on-screen text boxes,
resulting in short phrases (e.g. “Amplified emotions and better
understanding of them”, “Fear of unknown effects, since its [sic] not
studied”) or in one- or two-word responses (e.g. “Creativity”, “Better
mood”, “Illegal”, “Too Energetic”). The coding authors (TA and AC)
independently coded these benefits and challenges using the principles
of classic grounded theory [34,35,36].
Discrepant codes were periodically discussed until a final set of codes
was agreed upon (i.e. saturation was reached). These codes were
hierarchically built into three layers of abstraction: codes (level one)
were grouped under sub-categories (level two), which were grouped under
categories (level three). This hierarchy was iteratively discussed and
changes were agreed upon over five refining passes. We incorporated the
diction used by the respondents where possible to better reflect the
data-driven nature of the final codebook (see Additional file 1 and full online codebook; [37]).
Inter-rater
agreement was calculated separately for benefits and challenges and at
each level (code, sub-category, category). Agreement was above 85% at
every level (benefit code 85.1%, benefit sub-category 89.2%, benefit
category 92.6%; challenge code 85.7%, challenge sub-category 86.9%,
challenge category 88.5%). Each report was coded twice, once by each
coding author, and the sum of coded items in each category was halved;
as a result, the frequency of any given category can be a non-integer
value (e.g. 807.5 coded benefits, 603.5 coded challenges; “Empirical
codebook: benefits of microdosing” and “Empirical codebook: challenges
of microdosing” sections).
Participation
was voluntary under informed consent, in accord with the Declaration of
Helsinki, and was non-remunerative. The sample analysed in the present
study includes the 278 respondents that answered the MDBC questions
after indicating they had experience with microdosing LSD-only,
psilocybin-only, or both LSD and psilocybin; respondents that indicated
they used other substances to microdose (e.g. DMT, Salvia divinorum) are
not included in the present report, allowing us to focus our efforts on
the most commonly reported microdosing substances that are most likely
to be studied in future research. Recruitment was primarily via the
online forum “Reddit” (Reddit Inc, San Francisco, CA, USA). Reddit is an
online forum with self-organizing sub-groups, called “subreddits”,
which curate content for their “subscribers”. These subreddits discuss
topics of mutual interest, making these communities potential pools of
willing participants akin to other crowdsourcing approaches, e.g. Amazon
mTurk, CrowdFlower, Prolific [38].
Compared to the US population, Reddit users tend to be younger,
educated or seeking a college education, and present in a male-to-female
ratio of approximately 2:1 [39]
thus this sample’s generalizability is limited to modern Western
populations. In the present sample, respondents had a mean age of 27.8
(SD 8.9); age was non-normally distributed with an interquartile range
of 21–31 years (median 26.0, range 16–63). Most participants were male (M 237, F 31, other 10), heterosexual (N = 211, other 57), and white or European (N = 234,
other 44). For a more comprehensive breakdown of all survey
respondents, see our epidemiological report, which includes reports on
psychiatric disorders (Rosenbaum D, Weissman C, Hapke E, Hui K,
Petranker R, Dinh-Williams L-A, et al.: Microdosing psychedelic
substances: demographics, psychiatric comorbidities, and comorbid
substance use, in preparation). Microdosers from the following
subreddits were solicited: Microdosing, Nootropics, Psychonaut,
RationalPsychonaut, Tryptonaut, Drugs, LSD, shrooms, DMT,
researchchemicals, and SampleSize [40].
Respondents
completed a survey about their microdosing history including
microdosing regimen (substance, dose, etc.), subjective benefits and
challenges of microdosing, the importance of these benefits and
challenges, and focal questions concerning behaviour and consumption
changes. For concision, the numerous variables collected but not
discussed here are not described here; many are discussed in our
previous work [8]
(Rosenbaum D, Weissman C, Hapke E, Hui K, Petranker R, Dinh-Williams
L-A, et al.: Microdosing psychedelic substances: demographics,
psychiatric comorbidities, and comorbid substance use, in preparation)
and the complete survey is available online [41].
Here we focus on questions concerning microdosing benefits and
challenges (MDBCs), health behaviours, and substance-use changes.
Microdosing
respondents reported up to three benefits and three drawbacks of
microdosing psychedelics. They also gave each outcome a rating of
subjective importance on a sliding scale from 0 to 100 [42].
Microdosing
respondents indicated whether they had, as a result of microdosing,
experienced improvements in each of the following domains: mood,
anxiety, meditative practice, exercise, eating habits, and sleep. They
also indicated whether they had reduced their use of any of the
following substances: caffeine, alcohol, cannabis, tobacco, psychiatric
prescription medications, and illicit substances. These questions
appeared on the page after the open-ended benefits and challenges
questions to avoid contamination via priming.
Respondents
reported the substance they used to microdose and were removed if they
indicated using substances other than LSD or psilocybin. This sample
includes 278 respondents in three categories: LSD-only (N = 195), psilocybin-only (N = 50), and respondents that have microdosed with LSD and psilocybin (N = 33).
Grounded
theory analyses resulted in a total of 807.5 coded benefits of
microdosing. Taxonomy-building resulted in 46 codes organized into 21
sub-categories and 11 categories. The most frequently reported codes
were improved mood (12.8%), improved focus (10.0%), creativity (9.4%),
and improved energy (7.6%).
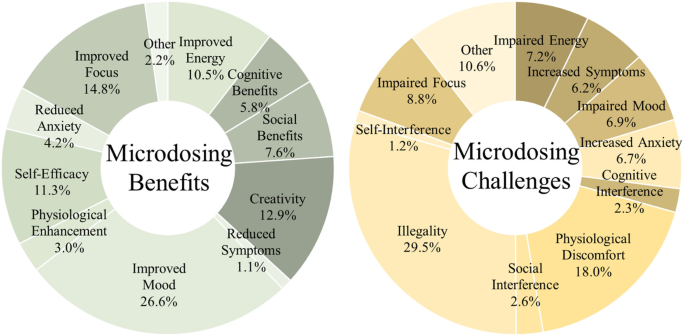
This summary provides descriptions of the 11 categories of benefits that were distiled from participant reports (Fig. 1).
As per grounded theory, the naming conventions for codes reflect the
language used by respondents, but more flexibility was introduced as
needed at higher orders of abstraction. Full descriptions of every code
are available in the full codebook (see Additional file 1).
Categories
of microdosing benefits and challenges. Values indicate percentage
endorsement of outcomes. Values were generated through open-ended
responses, and thus magnitude is descriptive and should be used for
hypothesis generation. These data indicate reported outcomes, not
confirmed effects
Improved
mood (26.6%, 215 reports): This most frequently reported
benefit-category captures all codes related to mood improvements:
happiness, well-being, peace, calm, and reductions in depressive
symptoms. Also included are reports of improved outlook, appreciation of
life, optimism, spiritual and emotional insights, and being more in
touch with emotions.
Improved focus (14.8%, 119.5 reports): This
benefit-category references codes concerning focus and concentration,
conscious awareness, mindfulness, and increased engagement and
attentiveness.
Creativity (12.9%, 104 reports): This category
includes creativity per se, as well as meta-creative processes, e.g.
shifting perspectives, divergent thinking, curiosity, and openness.
Self-efficacy
(11.3%, 91.5 reports): This category references improvements in
self-efficacy (motivation/ambition, productivity, confidence, sense of
agency) and self-care (introspection, meditation, and other behaviours
facilitating mental health).
Improved energy (10.5%, 84.5
reports): This category includes codes referencing “improved energy” per
se, as well as alertness, wakefulness, and stimulation.
Social
benefits (7.6%, 61 reports): This category references various socially
facilitating benefits such as extraversion, empathy, sense of
connection, and verbal fluency.
Cognitive benefits (5.8%, 47
reports): This category concerns cognitive enhancement (understanding,
problem-solving), clarity of thought (clear headedness, lucidity), and
memory.
Reduced anxiety (4.2%, 34 reports): References to anxiety reduction and social-anxiety reduction fit in this category.
Physiological
enhancement (3.0%, 24 reports): This category concerns biological
processes including enhanced senses (especially visual), cardiovascular
endurance, sleep quality, and reduced migraines and/or headaches.
Other
perceived benefits (2.2%, 18 reports): This category was a catch-all
for otherwise uncategorized codes. These include the novelty of the
experience itself, the ability to control the dose, the lack of
side-effects, and other miscellany. This category also includes 1 report
that there were no beneficial effects.
Reduced symptoms (other)
(1.1%, 9 reports): References to stress reduction, reduced sensitivity
to trauma, and references to reduced substance dependence (e.g. quitting
smoking) are included.
Grounded
theory coding resulted in a total of 603.5 coded challenges of
microdosing. Taxonomy-building resulted in 44 codes organized into 23
sub-categories and 11 categories. The most frequently reported low-level
codes were illegality (10.8%), dose accuracy (9.1%), poor focus (8.8%),
and anxiety (5.3%).
As above, this summary provides extended descriptions of the 11 categories of challenge (Fig. 1).
Illegality
(29.5%, 178 reports): This category captures codes concerning the
illegality of psychedelic microdosing substances per se, as well as
codes concerning the consequences thereof. These include dosing
challenges associated with unregulated substances (e.g. taking too much
or too little), the availability of the substance (i.e. dealing with the
black market), and cost of the substance. Also included is the social
stigma surrounding the use of these substances and feeling the need to
hide one’s activity from others.
Physiological discomfort (18.0%,
108.5 reports): This category concerns physically detrimental challenges
including disrupted senses (visual), temperature dysregulation,
numbing/tingling, insomnia, gastrointestinal distress, reduced appetite,
and increased migraines and/or headaches.
Impaired focus (8.8%,
53 reports): This challenge category references codes concerning poor
focus, distractibility, and absent-mindedness.
Increased anxiety (6.7%, 40.5 reports): References to increased anxiety (general, social, existential) fit in this category.
Impaired
energy (7.2%, 43.5 reports): This category includes codes referencing
both excessive energy (restlessness, jitters) and inadequate energy
(fatigue, drowsiness, brain fog).
Impaired mood (6.9%, 41.5
reports): This category includes codes related to mood deterioration
(sadness, discontent, irritability), emotional difficulties
(over-emotionality, mood swings), and impaired outlook (fear, feeling
unusual).
Social interference (2.6%, 15.5 reports): This category
references various socially impairing challenges such as awkwardness,
oversharing, and difficulties with sentence-production in social
settings.
Cognitive interference (2.3%, 14 reports): This category concerns confusion, disorientation, racing thoughts, and poor memory.
Self-interference
(1.2%, 7.5 reports): This category references codes concerning
self-processing concerns (dissociation, depersonalization) and
self-sabotaging (rumination, over-analysis).
Other perceived
challenges (10.6%, 64 reports): This category was a catch-all for
otherwise uncategorized codes. These include the unknown risk-effect
profile of microdosing itself, the need to prepare and remember to dose,
references specifically citing that there were no challenges (1.5%),
and other miscellany. This category also includes reports that there
were no beneficial effects (0.6%). Furthermore, this category includes
substance-related concerns regarding taste, pupil dilation, and duration
of effects, and also concerns about negative drug interactions.
Increased
symptoms (other) (6.2%, 37.5 reports): References to after effects
(psychological dependence and concerns about potential addiction,
substance tolerance, comedown or hangover) and also more concerning, but
rare, adverse psychological events (0.7%).
Subjective
importance ratings were non-normally distributed thus Wilcoxon signed
rank tests were used to compare between substances. There was a
significant difference between the subjective rated importance of
benefits based on substance (W = 3658, p < 0.01, N1 = 195, N2 = 50, d = 0.353)
with psilocybin-only microdosers (median = 87.83, SD = 15.76) rating
benefits as significantly more important than LSD-only microdosers
(median = 76.67, SD = 14.59); there were no differences found relative
to respondents using both LSD and psilocybin (median = 82.33,
SD = 14.28, ps > 0.14). The substance-related difference between
subjective importance of challenges was non-significant (W = 3841.5, p = 0.56, N1 = 177, N2 = 46, d = 0.079)
with psilocybin-only microdosers (median = 47.67, SD = 24.98) rating
challenges equivalently to LSD-only microdosers (median = 47.5,
SD = 24.65); there were no differences found relative to respondents
using both LSD and psilocybin (median = 51.67, SD = 23.79,
ps > 0.66). Rates at which specific MDBC categories were reported did
not differ between LSD-only, psilocybin-only, and LSD and psilocybin
respondents (benefits χ2(20) = 17.26, p = 0.636; challenges χ2(20) = 7.73, p = 0.994).
After
reporting open-ended outcomes, participants answered targeted questions
concerning behavioural improvements and substance-use reductions (Fig. 2).
Respondents reported improved mood (92.9%), anxiety (59.2%), meditative
practice (49.1%), exercise (49.1%), eating habits (36.0%), and sleep
(28.8%). They also indicated reduced use of caffeine (44.2%), alcohol
(42.3%), cannabis (30.3%), tobacco (21.0%), psychiatric prescription
medications (16.9%), and illicit substances (16.1%).
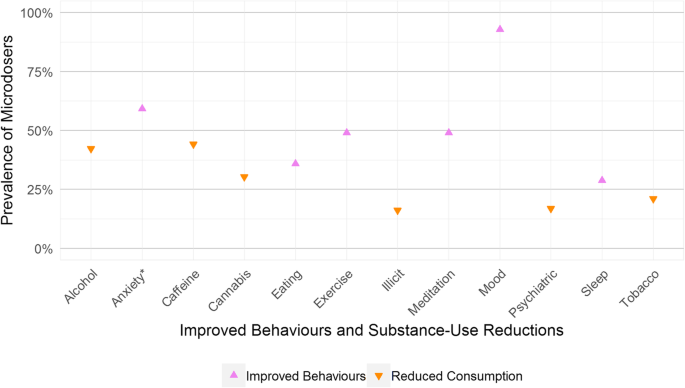
Percentage
of microdosers endorsing improved behaviours and reductions in
substance-use. Prevalence rate should be used for hypothesis generation
as these data indicate reported outcomes, not confirmed effects. *Note:
Anxiety refers to improvements to anxiety-related experiences, not to
increased experience of anxiety
Surveying
extant communities of microdosers allowed for the creation of an
initial qualitative taxonomy of MDBCs. These empirically-grounded MDBCs
can inform future microdosing research by leveraging participant reports
for high-potential intervention targets so research time and funding
can be efficiently allocated. For example, microdosers often report
changes in mood, focus, and creativity thus these constructs should be
targeted in future intervention research. Concerns of physiological
discomfort and restlessness were also commonly reported thus they should
also be monitored.
While the improvements and reductions reported
by respondents sound promising, they cannot be disentangled from
expectation and placebo effects or recall biasses. Furthermore, the MDBC
findings cannot indicate causation as this study was observational, not
experimental. With these caveats in mind, we discuss how researchers
can use these initial findings in their future studies. While
necessarily inconclusive due to their exploratory nature, these results
point to potential therapeutic effects warranting future
placebo-controlled microdosing research.
Major
parallels between benefits and challenges emerged among outcomes.
Specifically, each category of outcome is seen as both a benefit and a
challenge, other than creativity and illegality (Table 1).
This kind of mirroring suggests two hypotheses concerning microdosing:
(1) placebo effects and expectancy play a major role in reported effects
and/or (2) individual differences moderate reported effects.
The
first and most parsimonious hypothesis that could explain the
parallelism between benefits and challenges is that the effects cancel
out and nothing replicable is happening. The presence of opposite
outcomes with a net-zero effect is what might be expected in an inactive
condition dominated by noise. For example, if microdosing has no
effect, random variation might result in some participants reporting
decreased anxiety while others report increased anxiety. It may also be
the case that microdosing interacts with expectancy in some way,
enhancing the effect of expectancy and thus the outcomes could differ
even more than anticipated based on the mind-set of the microdoser.
Indeed, “set and setting” are major components of full-dose psychedelic
use and expectancy is understood to greatly alter the outcome potentials
of full-dose psychedelics [31].
Perhaps “set and setting” are also of importance in microdosing, though
this remains to be tested. Indeed, each of the constructs described in
this taxonomy should be directly tested in placebo-controlled trials.
Nevertheless,
there are plausible pharmacological mechanisms of action for
microdosing, and it is possible that individual differences in
genetically mediated substance metabolism, psychopathological diagnoses
and personality, and momentary interpretations of interoceptive signals
affect how microdosing outcomes manifest. The HTR2A gene, which encodes
the serotonin 5HT-2A receptor, can have various mutations [43]
which, alongside other genetic and epigenetic influences, play a role
in how 5HT-2A agonists, including LSD and psilocybin, are processed
neuropharmacologically. As such, individual differences in receptor
sensitivity may moderate optimal microdosing doses, substance choice,
and dosing schedule. Genetic and epigenetic factors also influence
psychopathology and personality, which can moderate responses to
psychedelics [44].
For example, a person with a mood disorder (e.g. major depression) may
find that microdosing has a different effect than a person scoring in
the healthy range on a depression inventory. One possibility is that
increasing between-network functional connectivity could disrupt the
patterned use of cortical networks overly favoured under a specific
pathology (e.g. to disrupt the greater functional connectivity between the DMN and subgenual prefrontal cortex seen in depression; [45]).
In contrast, altering the functional connectivity in a healthy brain
could plausibly produce undesirable activity rather than maintain
healthy network coherence [46, 47].
Indeed, even in non-pathological participants, top-down interpretations
of interoceptive events could cast physiological experiences (e.g.
arousal) in a negative light (e.g. restlessness) rather than a positive
one (e.g. wakefulness).
These different interpretations may be amenable
to intervention by preparing participants for certain physiological
outcomes [31]
whereas the genetic, epigenetic, and psychopathological features could
constitute more stable predictors. These moderation hypotheses remain
for future research.
While parallelism emerged, not all categories were equally reported on both sides of the benefit/challenge divide (Fig. 3).
When calculating the difference between how often categories of
benefits were reported versus how often the parallel challenge-category
was reported, the three largest differences in raw reporting rates were
mood being more often improved (215 as benefit versus 41.5 as
challenge), self-efficacy being more often increased (91.5 benefit, 7.5
challenge), and physiological response being more often discomforting
(24 benefit, 108.5 challenge). These categories may provide especially
promising starting points for future microdosing research. Anxiety was
closest to even with the difference being only 6.5 reports (34 benefit,
40.5 challenge).
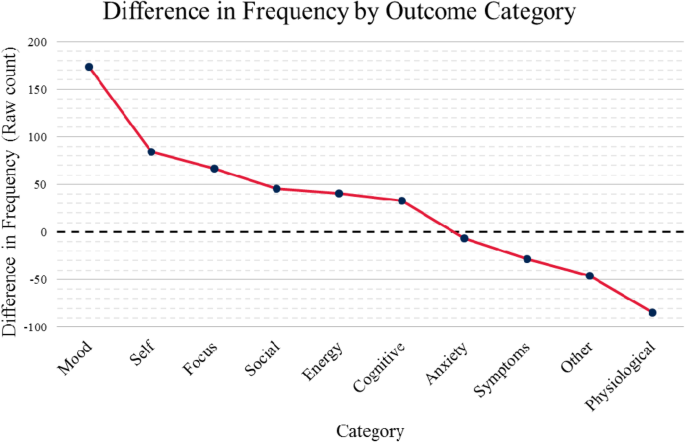
Difference
in raw count of reported benefits and challenges. Positive values
indicate greater endorsement of benefits in the indicated category;
negative values reflect greater endorsement of challenges. Comparisons
are exploratory thus differences, regardless of magnitude, should be
used for hypothesis generation. These data indicate perceived outcomes
and do not indicate confirmed effects
Parallelism
between benefits and challenges was not universal. The taxonomy
includes both unique beneficial and detrimental outcomes: (1) creativity
and (2) illegality.
Creativity was the third most common benefit
category, and there was no opposite challenge (i.e. participants did not
report that microdosing made them less creative or more closed-minded).
Microdosers report enhanced creativity and meta-creative processes,
such as perspective-shifting/divergent thinking and openness/curiosity.
These findings accord with other findings that microdosers have higher
creativity than non-microdosers [8, 11] and with full-dose research showing increased openness after full-dose psilocybin [24]. Early psychedelic research preliminarily investigated creativity enhancement and problem-solving [48],
and this exciting topic could again be subject to study. Future studies
should initially measure various aspects of creativity—e.g. divergent
thinking, convergent thinking, insight [8, 11, 49, 50]—to inform more focal investigations on how microdosing may affect creativity.
Illegality
was the most commonly reported microdosing challenge. It is notable
that the most frequently reported “outcome” is a socio-cultural
circumstance, not an outcome of microdosing per se. Psychedelics were
made illegal by the UN Convention on Psychotropic Substances in 1971 and
remain so today [13, 51]. Illegality has resulted in a thriving black market economy for illicit substances, both in-person and online [52].
This unregulated criminal market results in unpredictable substance
purity, dose accuracy, supply availability, and cost. Illegality has
further societal consequences, namely the social stigma associated with
substance use, even though psychedelic substances have a relatively
benign safety profile compared to other substances, including several
legal substances [53]. As such, researchers have begun calling for the legal rescheduling of psychedelic substances [54].
In addition to the emergent qualitative categories, participants reported on several a priori focal outcomes (Fig. 2).
Nine-tenths of respondents endorsed that microdosing improved their
mood, which is in agreement with improved mood being the most commonly
reported benefit-category. Anxiety improvement was also notable with 59%
of respondents indicating this benefit. These rates of reported
improvement suggest future research into microdosing for mood and
anxiety may be warranted, complementing the recent work treating
depression and anxiety with psilocybin [19, 20].
Participants also indicated decreased use of caffeine, alcohol, cannabis, and tobacco (Fig. 2). These findings align with research on full-dose psychedelics: LSD and psilocybin may promote reduced alcohol abuse [14, 16], and psilocybin can have potent long-term reductions in smoking [55].
Microdosing could be investigated as a potential complement,
supplement, or alternative to full-dose interventions for smoking
cessation or substance use disorders.
The
intent of the present study was to inform empirically-grounded
data-collection initiatives by providing high-potential outcomes
deserving of further study, while also showcasing challenges that
warrant measurement and suitable caution. The intent of the present
study was not to make causal claims. We employed no experimental
manipulation or longitudinal component, could not control for substance
purity, schedule, or dose, nor for prior experience with full-dose
psychedelics, and we cannot account for recall bias or placebo effects.
MDBCs described here reflect the reports of microdosers, but we cannot
claim that these perceived outcomes are causally related to microdosing.
LSD and psilocybin were the most frequently used substances and, as
microdosing continues to be culturally, scientifically, and clinically
relevant, it will be important to establish dose-dependent outcomes of
microdosing and to consider the different contexts in which micro- and
full doses may be variably appropriate, including when they may
complement each other.
Our participant recruitment strategy relied
on self-selection and sampled primarily from Reddit; this strategy may
have introduced demographic biasses, and these data should not be
considered epidemiologically definitive (see Rosenbaum et al. (Rosenbaum
D, Weissman C, Hapke E, Hui K, Petranker R, Dinh-Williams L-A, et al.:
Microdosing psychedelic substances: demographics, psychiatric
comorbidities, and comorbid substance use, in preparation) for further
discussion). More than 70% of the sample reported countries of
Anglo-cultural origin, and this sample is limited in the sense that it
does not reflect a random sampling of the human population. We sought a
sample of psychedelic microdosers, a group that may not be randomly
distributed in the population, thus this convenience sample is still
informative. Nevertheless, future intervention work should endeavour to
recruit more inclusive and representative samples.
Qualitative
research is, by its nature, biassed by the research team and their
coding decisions. MDBCs were processed by two interdependent coders (TA
and AC) that iteratively constructed the agreed-upon codebook.
Hypothesis-driven coding was avoided to maintain code-integrity [36] and, supporting transparency and re-analysis, both the coded and raw data have been made available [41].
Another taxonomy could emerge from different investigators pursuing
more targeted research questions, so these MDBCs should not be taken as
definitive. The present taxonomy offers a foundation from which future
focal research can be built.
Ultimately, pre-registered randomized
placebo-controlled trials (RCTs) of microdosing psychedelics are needed
to test its safety and efficacy. Using the MDBC taxonomy as a starting
point, appropriate measures can be included to investigate the causal
outcomes of microdosing and the mechanisms underlying those outcomes.
The potential of microdosing is not yet well understood, but the
benefits reported in this taxonomy suggest potential novel research
avenues for psychedelic-based pharmacotherapeutic treatment of
depression, anxiety, ADHD, smoking cessation, and substance use
disorders. Exploring the potential of microdosing for creativity is also
warranted.
Here
we provide an initial taxonomy of benefits and challenges associated
with psychedelic microdosing, which compliments the other reports built
from this larger microdosing research project [8]
(Rosenbaum D, Weissman C, Hapke E, Hui K, Petranker R, Dinh-Williams
L-A, et al.: Microdosing psychedelic substances: demographics,
psychiatric comorbidities, and comorbid substance use, in preparation).
The findings presented here suggest a number of potential microdosing
research avenues, though experimental, hypothesis-driven studies are
needed. The MDBC taxonomy, behavioural improvements, and substance-use
reductions warrant RCTs to test therapeutic safety and efficacy of
microdosing psychedelics. Online microdosing communities have grown to
the tens of thousands, speaking to a social need for scientific study to
inform the public about the effects of microdosing. Microdosing
research could help inform future psychedelic research by investigating
the potential for mixing or contrasting micro- and full-dose psychedelic
psychotherapies. We call researchers to do this work following the
principles of open science and share our resources accordingly [41].
After a 40-year moratorium, the psychedelic renaissance has begun:
rigorous scientific methods can now be used to investigate psychedelics
as potential medicines and for “the betterment of well people” [1].
The dataset supporting the conclusions of this article is available on the Open Science Framework (osf.io/g5cwy/).
- Pollan M. The trip treatment. 2015 [cited 2018 Nov 16]; Available from: https://www.newyorker.com/magazine/2015/02/09/trip-treatment
- Pollan M. How to change your mind: what the new science of psychedelics teaches us about consciousness, dying, addiction, depression, and transcendence: Penguin; 2018. p. 558.
- Leonard A. How LSD microdosing became the hot new business trip. Rolling Stone. 2015 [cited 2018 Jul 9]. Available from: https://www.rollingstone.com/culture/culture-news/how-lsd-microdosing-became-the-hot-new-business-trip-64961/
- Solon O. Under pressure, Silicon Valley workers turn to LSD microdosing. Wired UK. 2016 [cited 2018 Jul 9]; Available from: http://www.wired.co.uk/article/lsd-microdosing-drugs-silicon-valley
- Anderson T, Petranker R. “Microdosers” of LSD and magic mushrooms are wiser and more creative. The Conversation. 2018 [cited 2018 Nov 14]. Available from: http://theconversation.com/microdosers-of-lsd-and-magic-mushrooms-are-wiser-and-more-creative-101302
- Eligh B. Rethinking psychedelics: U of T study looks at the practice of microdosing to ease anxiety and sharpen focus. University of Toronto News. 2018 [cited 2018 Aug 29]; Available from: https://www.utoronto.ca/news/rethinking-psychedlics-u-t-study-looks-practice-microdosing-ease-anxiety-and-sharpen-focus
- Ghosh I. How and why people “microdose” tiny hits of psychedelic drugs. CBC. 2018 [cited 2018 Aug 29]; Available from: https://www.cbc.ca/news/health/microdosing-pschedelics-study-1.4771647
- Anderson T, Petranker R, Rosenbaum D, Weissman CR, Dinh-Williams L-A, Hui K, et al. Microdosing psychedelics: personality, mental health, and creativity differences in microdosers. Psychopharmacology (Berl). 2019 [cited 2019 Jan 2]; Available from: https://doi.org/10.1007/s00213-018-5106-2
- Johnstad PG. Powerful substances in tiny amounts: an interview study of psychedelic microdosing. Nord Stud Alcohol Drugs. 2018;35(1):39–51.
- Polito V, Stevenson D. A systematic study of microdosing psychedelics. PsyArXiv. 2018 [cited 2018 Jul 5]; Available from: https://psyarxiv.com/cw9qs/
- Prochazkova L, Lippelt DP, Colzato LS, Kuchar M, Sjoerds Z, Hommel B. Exploring the effect of microdosing psychedelics on creativity in an open-label natural setting. Psychopharmacology (Berl). 2018 [cited 2018 Oct 25]; Available from: https://doi.org/10.1007/s00213-018-5049-7
- Grinspoon L, & Bakalar JB. Psychedelic drugs reconsidered. New York: Basic Books. 1979;221–223.
- United Nations. The International Drug Control Conventions. 2013;10.
- Krebs TS, Johansen P-Ø. Lysergic acid diethylamide (LSD) for alcoholism: meta-analysis of randomized controlled trials. J Psychopharmacol (Oxf). 2012;26(7):994–1002.
- Johnson MW, Garcia-Romeu A, Cosimano MP, Griffiths RR. Pilot study of the 5-HT2AR agonist psilocybin in the treatment of tobacco addiction. J Psychopharmacol Oxf Engl. 2014;28(11):983–92.
- Bogenschutz MP, Forcehimes AA, Pommy JA, Wilcox CE, Barbosa PCR, Strassman RJ. Psilocybin-assisted treatment for alcohol dependence: a proof-of-concept study. J Psychopharmacol Oxf Engl. 2015;29(3):289–99.
- Noorani T, Garcia-Romeu A, Swift TC, Griffiths RR, Johnson MW. Psychedelic therapy for smoking cessation: qualitative analysis of participant accounts. J Psychopharmacol (Oxf). 2018;32(7):756–69.
- Rucker JJ, Jelen LA, Flynn S, Frowde KD, Young AH. Psychedelics in the treatment of unipolar mood disorders: a systematic review. J Psychopharmacol (Oxf). 2016;30(12):1220–9.
- Carhart-Harris RL, Bolstridge M, Day CMJ, Rucker J, Watts R, Erritzoe DE, et al. Psilocybin with psychological support for treatment-resistant depression: six-month follow-up. Psychopharmacology (Berl). 2018;235(2):399–408.
- Griffiths RR, Johnson MW, Carducci MA, Umbricht A, Richards WA, Richards BD, et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: a randomized double-blind trial. J Psychopharmacol Oxf Engl. 2016;30(12):1181–97.
- Ross S, Bossis A, Guss J, Agin-Liebes G, Malone T, Cohen B, et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. J Psychopharmacol Oxf Engl. 2016;30(12):1165–80.
- Reiche S, Hermle L, Gutwinski S, Jungaberle H, Gasser P, Majić T. Serotonergic hallucinogens in the treatment of anxiety and depression in patients suffering from a life-threatening disease: a systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2018;81:1–10.
- Mithoefer MC, Mithoefer AT, Feduccia AA, Jerome L, Wagner M, Wymer J, et al. 3,4-methylenedioxymethamphetamine (MDMA)-assisted psychotherapy for post-traumatic stress disorder in military veterans, firefighters, and police officers: a randomised, double-blind, dose-response, phase 2 clinical trial. Lancet Psychiatry. 2018;5(6):486–97.
- MacLean KA, Johnson MW, Griffiths RR. Mystical experiences occasioned by the hallucinogen psilocybin lead to increases in the personality domain of openness. J Psychopharmacol Oxf Engl. 2011;25(11):1453–61.
- Griffiths RR, Johnson MW, Richards WA, Richards BD, McCann U, Jesse R. Psilocybin occasioned mystical-type experiences: immediate and persisting dose-related effects. Psychopharmacology (Berl). 2011;218(4):649–65.
- Liechti ME. Modern Clinical Research on LSD. Neuropsychopharmacology. 2017;42:2114.
- Hendricks PS. Awe: a putative mechanism underlying the effects of classic psychedelic-assisted psychotherapy. Int Rev Psychiatry. 2018;30(4):331–42.
- Halpern JH, Pope HG. Do hallucinogens cause residual neuropsychological toxicity? Drug Alcohol Depend. 1999;53(3):247–56.
- van Amsterdam J, Opperhuizen A, van den Brink W. Harm potential of magic mushroom use: a review. Regul Toxicol Pharmacol. 2011;59(3):423–9.
- Johnson MW, Griffiths RR, Hendricks PS, Henningfield JE. The abuse potential of medical psilocybin according to the 8 factors of the Controlled Substances Act. Neuropharmacology. 2018;142:143–66.
- Johnson MW, Richards WA, Griffiths RR. Human hallucinogen research: guidelines for safety. J Psychopharmacol Oxf Engl. 2008;22(6):603–20.
- Carbonaro TM, Bradstreet MP, Barrett FS, MacLean KA, Jesse R, Johnson MW, et al. Survey study of challenging experiences after ingesting psilocybin mushrooms: acute and enduring positive and negative consequences. J Psychopharmacol (Oxf). 2016;30(12):1268–78.
- Johnson MW, Sewell RA, Griffiths RR. Psilocybin dose-dependently causes delayed, transient headaches in healthy volunteers. Drug Alcohol Depend. 2012;123(1–3):132–40.
- Corbin JM. Grounded theory. J Posit Psychol. 2017;12(3):301–2.
- Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual Sociol. 1990;13(1):3–21.
- Stol K, Ralph DP, FitzGerald B. Grounded theory in software engineering research: a critical review and guidelines. In 2016 [cited 2017 Mar 30]. Available from: https://researchspace.auckland.ac.nz/handle/2292/29124
- Anderson T, Petranker R, Dinh-Williams L-A. An empirical codebook of microdosing benefits and challenges [Internet]. 2018 [cited 2018 Dec 20]. Available from: https://osf.io/qwu4s/
- Peer E, Brandimarte L, Samat S, Acquisti A. Beyond the Turk: alternative platforms for crowdsourcing behavioral research. J Exp Soc Psychol. 2017;70:153–63.
- Sattelberg W. The demographics of Reddit: who uses the site?. Tech Junkie. 2018 [cited 2018 Aug 22]. Available from: https://www.techjunkie.com/demographics-reddit/
- Anderson T. Reddit user “oredna”, Thomas Anderson, PhD Student. reddit. 2017 [cited 2018 Sep 9]. Available from: https://www.reddit.com/user/oredna/
- Anderson T, Petranker R, Dinh-Williams L-A. Demography of microdosing community survey. Open Science Framework. 2017 [cited 2018 Jul 6]. Available from: https://osf.io/g5cwy/
- Matejka J, Glueck M, Grossman T, Fitzmaurice G. The effect of visual appearance on the performance of continuous sliders and visual analogue scales. In: Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems. New York: ACM; 2016. p. 5421–5432. (CHI ’16). [cited 2017 Jun 13] Available from: http://doi.acm.org/10.1145/2858036.2858063
- National Library of Medicine (US). Genetics home reference. HTR2A gene. 2018 [cited 2018 Nov 15]. Available from: https://ghr.nlm.nih.gov/gene/HTR2A
- Barrett FS, Johnson MW, Griffiths RR. Neuroticism is associated with challenging experiences with psilocybin mushrooms. Personal Individ Differ. 2017;117:155–60.
- Hamilton JP, Farmer M, Fogelman P, Gotlib IH. Depressive rumination, the default-mode network, and the dark matter of clinical neuroscience. Biol Psychiatry. 2015;78(4):224–30.
- Bowyer SM. Coherence a measure of the brain networks: past and present. Neuropsychiatr Electrophysiol. 2016;2(1):1.
- Decker S, Fillmore PT, Roberts A. Coherence: The measurement and application of brain connectivity. NeuroRegulation. 2017;4(1):3.
- Harman WW, McKim RH, Mogar RE, Fadiman J, Stolaroff MJ. Psychedelic agents in creative problem-solving: a pilot study. Psychol Rep. 1966;19(1):211–27.
- Lin W-L, Hsu K-Y, Chen H-C, Chang W. Different attentional traits, different creativities. Think Ski Creat. 2013;9:96–106.
- Webb ME, Little DR, Cropper SJ. Insight is not in the problem: investigating insight in problem solving across task types. Front Psychol. 2016 [cited 2018 Jun 2];7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5035735/
- UNODC. Final act of the United Nations conference for the adoption of a protocol on psychotropic substances. In: The International Drug Control Conventions. United Nations Office on Drugs and Crime; 2013. p. 71–75. [cited 2018 Aug 9] Available from: http://www.un-ilibrary.org/drugs-crime-and-terrorism/the-international-drug-control-conventions_814e78a6-en
- Taylor H. Hit men, drugs and malicious teens: the darknet is going mainstream. CNBC. 2016 [cited 2018 Aug 9]; Available from: https://www.cnbc.com/2016/05/18/hit-men-drugs-and-malicious-teens-the-darknet-is-going-mainstream.html
- Nutt DJ, King LA, Phillips LD. Drug harms in the UK: a multicriteria decision analysis. Lancet. 2010;376(9752):1558–65.
- Rucker JJH. Psychedelic drugs should be legally reclassified so that researchers can investigate their therapeutic potential. BMJ. 2015;350:h2902.
- Johnson MW, Garcia-Romeu A, Griffiths RR. Long-term follow-up of psilocybin-facilitated smoking cessation. Am J Drug Alcohol Abuse. 2017;43(1):55–60.
No comments:
Post a Comment