
This study investigates the plausibility of applying continuous low doses of DMT for therapeutic purposes. so far so good. This is basic research long overdue.
There will be safe therapeutic levels and there will be safe recreational levels as well. Both are worthy of study and experience evaluation as well to see what we can gain over a significant population.
This all welcome even if the outcome makes it an unsatisfactory drug for any usage. at least then we will know what is possible and why.
.
A Model for the Application of Target-Controlled Intravenous Infusion for a Prolonged Immersive DMT Psychedelic Experience
- 1Computational Neuroscience Unit, Okinawa Institute of Science and Technology Graduate University, Okinawa, Japan
- 2Department of Psychiatry, University of New Mexico School of Medicine, Albuquerque, NM, USA
http://journal.frontiersin.org/article/10.3389/fphar.2016.00211/full
The state of consciousness induced by N,N-dimethyltryptamine
(DMT) is one of the most extraordinary of any naturally-occurring
psychedelic substance. Users consistently report the complete
replacement of normal subjective experience with a novel “alternate
universe,” often densely populated with a variety of strange objects and
other highly complex visual content, including what appear to be
sentient “beings.” The phenomenology of the DMT state is of great
interest to psychology and calls for rigorous academic enquiry. The
extremely short duration of DMT effects—less than 20 min—militates
against single dose administration as the ideal model for such enquiry.
Using pharmacokinetic modeling and DMT blood sampling data, we
demonstrate that the unique pharmacological characteristics of DMT,
which also include a rapid onset and lack of acute tolerance to its
subjective effects, make it amenable to administration by
target-controlled intravenous infusion. This is a technology developed
to maintain a stable brain concentration of anesthetic drugs during
surgery. Simulations of our model demonstrate that this approach will
allow research subjects to be induced into a stable and prolonged DMT
experience, making it possible to carefully observe its psychological
contents, and provide more extensive accounts for subsequent analyses.
This model would also be valuable in performing functional neuroimaging,
where subjects are required to remain under the influence of the drug
for extended periods. Finally, target-controlled intravenous infusion of
DMT may aid the development of unique psychotherapeutic applications of
this psychedelic agent.
Introduction
N,N-dimethyltryptamine (DMT) produces some of the
most extraordinary changes in consciousness of any naturally-occurring
psychedelic substance. Users consistently report the complete
replacement of awareness of the normal waking world with a bizarre and
complex “alternate universe” filled with a variety of visual objects,
including what appear to be sentient, intelligent, and powerful
“beings,” many of which actively interact with the individual (Strassman, 2001, 2008; Luke, 2011; Gallimore, 2013). Furthermore, the endogenous production of DMT in humans is well-established (Barker et al., 2012),
although the biological significance of this remains to be elucidated.
DMT is actively transported across the blood brain barrier in rats and
dogs (Sangiah et al., 1979; Takahashi et al., 1985; Yanai et al., 1986),
and a similar mechanism plausibly exists in humans. DMT is also a
substrate for the human serotonin and monoamine vesicular transporters (Cozzi et al., 2009).
The key enzyme for its production, indolethylamine N-methyltransferase,
has been detected in the brain, pineal gland, and retina of primates (Cozzi et al., 2011).
Taken together, these data suggest that DMT may have a significant role
in human neurophysiology, consciousness, and the visual system.
Clinical psychedelic drug research has resumed after a
generation's hiatus, and its scope is expanding rapidly. Modern
functional neuroimaging techniques are revealing the neural
accompaniment of these altered states of consciousness (Vollenweider et al., 1997; Carhart-Harris et al., 2012; Roseman et al., 2014; Tagliazucchi et al., 2014; Gallimore, 2015; Nichols, 2016).
However, comparable thoroughgoing analyses of their phenomenology are
lacking. This is surprising because of how unusual and highly replicable
are the subjective effects of the psychedelic drugs in general, in
particular those of DMT. The profound and easily reproducible effects of
DMT and other psychedelics may provide valuable insights into the
structure of the human mind—the central focus of psychology itself. As
such, in addition to their neural correlates, the phenomenology and
content of the DMT state calls for rigorous academic enquiry.
Studies of DMT in humans began in the 1950s (Boszormenyi and Szara, 1958; Sai-Halasz et al., 1958; Szara, 2007; Gallimore and Luke, 2015),
when its mind-altering effects were explored as a form of
chemically-induced psychosis. However, such studies simply classified
the complex visual effects as “hallucinations” with no further analysis.
Neither do most modern studies purporting to examine the psychological
effects of psychedelic drugs routinely provide detailed descriptions of
the altered state (Riba et al., 2001; Gouzoulis-Mayfrank et al., 2005).
An exception is the largest clinical study of DMT to date, which paid
careful attention to the content of the DMT experiences of nearly five
dozen volunteers administered a wide range of DMT doses (Strassman et al., 1994; Strassman, 1995, 2001).
The time course of DMT administered via inhalation of
vaporized freebase or intravenous injection of a water-soluble salt is
brief. The onset is rapid and overwhelming, with full effects noted
within 2 min of administration. Subjective effects are usually fully
resolved within 20–30 min. A powerful “rush” heralds the effect of a
fully psychedelic dose of DMT, marked by a sense of tremendous
acceleration and psychic and somatic tension. These culminate in the
dissociation of consciousness from bodily awareness and entry into a
“world of light” characterized by extremely complex visions. Users
frequently report the sense of receiving “information,” as well as the
conviction that what is being observed feels as if it were an autonomous
alternate world rather than a dream or hallucination. A commonly heard
refrain is that the experience was “more real than real.”
The inability to induce psychological tolerance to
repeated full-psychedelic doses of intravenous DMT administered by bolus
injection (Strassman et al., 1996) makes it unique among classic serotonergic psychedelics: e.g., LSD (Belleville et al., 1956).
This property renders DMT amenable to administration by continuous
intravenous infusion, in which the drug is administered at a
predetermined rate over a period of time and subjective effects can be
prolonged.
Gouzoulis-Mayfrank et al. (2005)
used such an approach to study the psychological effects of both DMT
and ketamine. This group's infusion rates were established by observing
the subjective effects of the drug, rather than taking into account its
underlying pharmacokinetics or pharmacodynamics. That three of the 15
subjects dropped out of the study because of adverse psychological
reactions suggests that this model resulted in an overly high infusion
rate. A more pharmacokinetically-informed approach to infusion will
allow the attainment and maintenance of a stable blood—and presumably
brain—concentration of DMT, and thus provide a safe and effective
prolonged immersion in the unique DMT state.
Methods and Results
Target-controlled intravenous infusion is a methodology
developed for use in general anesthesia, during which it is essential
that the concentration of drug at the target site (the brain) be
established and stably maintained (Kenny and White, 1990; Absalom et al., 2016).
If drug levels drop too low, the patient may rouse during the
procedure, and rising brain levels may result in potentially
life-threatening effects. Computer-assisted infusion devices are now
routinely used to ensure anesthetic levels remain within the required
therapeutic window. The foundation of these systems is a mathematical
model of the pharmacokinetics and pharmacodynamics of the anesthetic
drug (Gambus and Troconiz, 2015).
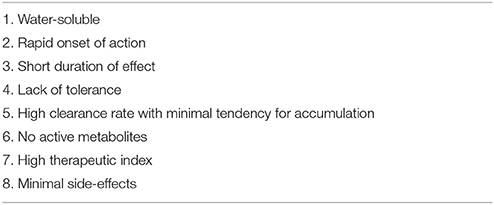
For a drug to be suitable for target-controlled infusion it should
ideally possess a number of characteristics listed in Table 1 (Miller, 1994). Fortunately, the water-soluble DMT salt used for intravenous administration meets all of these criteria.
TABLE 1
As a drug is introduced into the body
by intravenous injection, it is rapidly diluted and distributed by the
blood. It also equilibrates to various degrees with peripheral
tissues—dependent on specific drug properties and degree of
vascularization of the relevant tissues—and with the effect site itself.
The elimination of the drug from the body also begins immediately, by a
combination of enzymatic transformation, and urinary and/or biliary
excretion. Pharmacokinetic models must take into account both intrinsic
and drug-specific factors that affect drug absorption, distribution, and
elimination. Single-compartment models only consider the rapid dilution
of the drug in the main vascular compartment, whereas two- and three-
compartment models also take into account equilibration of the drug with
peripheral tissues. The pharmacokinetics of most anesthetics are best
fitted to either a two- or three-compartment model (Shafer and Gregg, 1992). Since DMT turns out to be best fitted to a two-compartment model (see later), only this type will be described here (Figure 1).
FIGURE 1
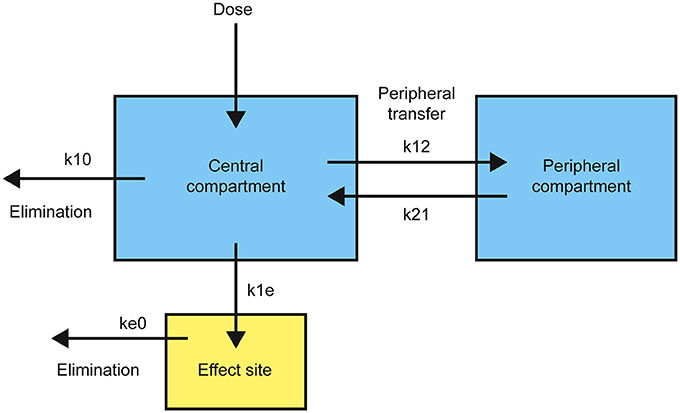
Figure 1. Structure of a standard two-compartment (plus effect site) pharmacokinetic model with transfer and elimination rates.
Drug is introduced into the central compartment to rapidly achieve a plasma concentration, CT, dependent on the volume of distribution, VC.
The drug is removed from the central compartment, quantified by a drop
in plasma concentration over time, by both elimination and equilibration
with the peripheral compartment. This rate of plasma concentration
decline is controlled by the elimination rate constant, k10, and the relative rates of movement from the central to the peripheral compartment, k12, and in the opposite direction, k21. The overall rate, RT, obeys the differential equation:
Complete equilibration with the peripheral compartment
is reflected in the exponential term decaying to zero and the steady
state elimination rate, RSS, is:
Transfer from the central compartment to the effect site, R1E, is generally modeled as a first-order process with rate constant, k1e:
To maintain a constant plasma, and thus effect site, concentration, the infusion rate must equal the overall removal rate, RT. Since this is not constant, except at steady state, the infusion rate must be adjusted to approximate the decline in RT over time. This requires the determination of the pharmacokinetic parameters: VC, k10, k12, and k21, which can be achieved by fitting time-series blood sampling data to a pharmacokinetic model.
To establish that the pharmacokinetics of DMT make it
suitable for target-controlled infusion, we used DMT plasma
concentration data from a previous study (Strassman and Qualls, 1994).
The details are provided in the original paper. Briefly, each subject
receiving a “fully psychedelic” dose of DMT was administered either 0.2
or 0.4 mg/kg DMT fumarate over 30 s through an indwelling forearm
intravenous catheter, followed by a 15 s flush with sterile saline.
Blood samples were drawn before the infusion and at 2, 5, 10, 15, 30,
and 60 min from the end of the infusion (45 s after the infusion began).
Plasma DMT concentration in each sample was then determined using gas
chromatography-mass spectrometry (GC-MS). A total of nine subjects were
used in the analysis (9 sets each of 0.4 and 0.2 mg/kg time series
data).
These time-series data were fitted to one-, two-, and
three-compartment pharmacokinetic models. The naïve averaged data
approach is the most straightforward technique for fitting
pharmacokinetic data, in which plasma concentration at each time point
is averaged over all subjects to generate a mean dose-response curve.
This curve is then fitted to a pharmacokinetic model. However, methods
taking into account both fixed and random effects on the
dose-response—for example, non-linear mixed effects modeling
(NON-MEM)—often give more reliable parameter estimates. These methods
also allow identification of parameter covariates, such as weight or age
(Mould and Upton, 2012).
Using the Matlab Simbiology toolkit (Mathworks, Inc.), we
fitted the 0.2 and 0.4 mg/kg time- series data separately. Both
datasets were best fitted to a two-compartment model with enzymatic
clearance, consistent with Michaelis-Menten kinetics (Figure 2). This comports with the well-established rapid metabolism of DMT by monoamine oxidase (MAO) A (Barker et al., 1980; Sitaram et al., 1987; Riba et al., 2015). Table 2 shows the population parameter estimates obtained.
FIGURE 2
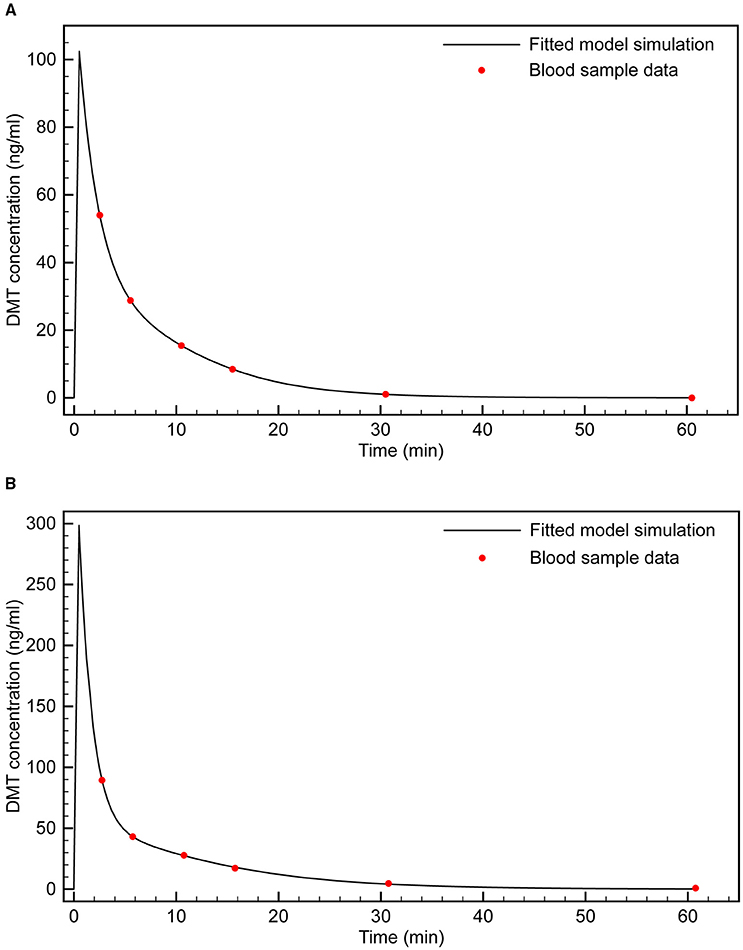
Figure 2. Fitting of two-compartment model with enzymatic clearance to blood sample data. (A) 0.4 mg/kg bolus; (B) 0.2 mg/kg bolus.
TABLE 2
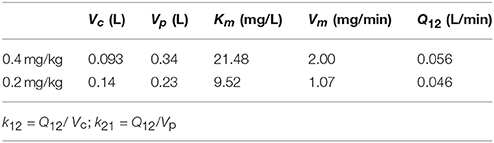
Table 2. Fitted pharmacokinetic parameters for 2-compartment model with enzymatic clearance.
These parameter estimates are for
an “average” individual (i.e., obtained from the mean plasma
concentration across the nine subjects at each time point), although the
dose-concentration response varied considerably among subjects. The
mean coefficients of variation in plasma DMT concentration, between 2
and 30 min post-infusion, across the 0.2 and 0.4 mg/kg groups were 83
and 58%, respectively. There was also variation in the estimated
parameters depending on the dose. Since 0.4 mg/kg was the most reliable
dose for inducing the fully psychedelic DMT experience, we sought an
infusion model that reaches and maintains the effect site concentrations
observed with this dose. Therefore, the 0.4 mg/kg parameter set was
chosen for development of the infusion model. However, comparable
results were obtained using the alternative parameter set.
Having established the model parameters, we then sought
to extend the model to include the effect site (brain) concentration.
The model was simulated using an infusion protocol employed in the
original study (i.e., 0.4 mg/kg infusion over 30 s). While subjects were
unable to communicate during the peak DMT effects, a number of
observations indicated that these peak effects in each subject occurred
at approximately 3 min from the beginning of the infusion. First, the
lower doses of drug (0.05 and 0.1 mg/kg) were not incapacitating, and
provided the opportunity for volunteers to describe the onset, peak, and
dissipation of drug effects in a running commentary narrative as they
were occurring. With these lower doses, effects peaked at approximately 3
min, began dissipating quickly, and were resolved by 15–20 min. That
the time course of peak DMT blood levels is identical across the
spectrum of doses suggests that the correspondence between the time
course of peak DMT effects and peak plasma levels at higher
incapacitating doses also holds true. Acute autonomic responses to DMT
also reached their highest levels between 2 and 5 min from the end of
the infusion, usually at the former time point. These included pupil
diameter, heart rate, and mean arterial blood pressure.
At the peak effect time, the drug concentration in the
central compartment is equal to the concentration at the effect site.
This makes it straightforward to model the effect site concentration
using the first-order rate equations:
where R1E is the rate of transfer of the drug from the central compartment to the effect site and RE0 is the elimination rate from the effect site, controlled by the rate constants k1e and ke0,
respectively. The parameters were tuned such that the peak effect site
concentration was reached at ~3 min. The resulting simulation is plotted
in Figure 3 and seems to fit the observations well.
FIGURE 3
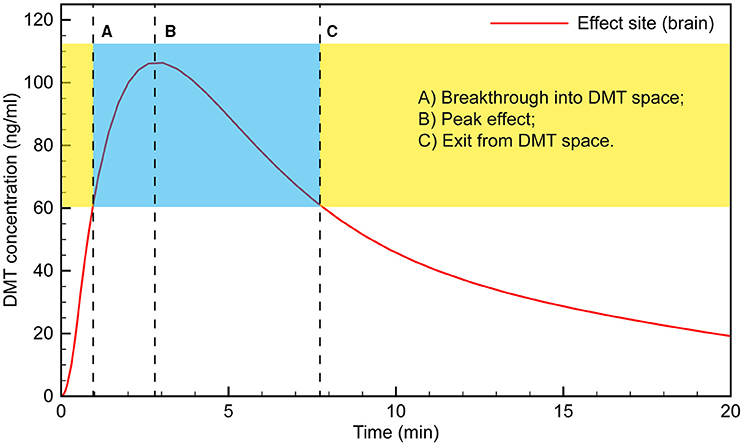
Figure 3. Simulated time course of DMT brain concentration following a 0.4 mg/kg bolus.
Typically, the subject would
appear to transition into full dissociation from the external world
toward the end of the 15 s saline flush following the 30 s DMT infusion.
This suggests that “breakthrough” into the DMT space occurs when the
effect site concentration reaches ~60 ng/ml. The subject then remains in
the “space” for the next 6–7 min, with the peak effect occurring at 3
min, when the effect site concentration is just over 100 ng/ml.
Clinical observation of the subjects appears to match
this time course, with their maximum level of absorption in the
subjective experience occurring at 4–5 min, likely as the initial rush
and disorientation began to subside. For example, subjects demonstrated
seemingly involuntary deep rhythmic breathing, the mouth being open in a
passive regressed manner, and REM-like eye movements behind closed
lids. Conversely, subjects appeared to be less under the influence of a
high dose of DMT as early as 5 min; e.g., moving their fingers, licking
their lips or yawning, taking a deep sighing breath, and stretching
their feet, suggesting that the acute drug effect was beginning to
lighten. Tellingly, almost every volunteer did not remember the 2 min
blood pressure measurement, whereas almost all remembered the 5 min
measurement, which is when our model suggests the effect site
concentration was again approaching ~60 ng/ml, when exit from the full
DMT intoxication occurs.
Having simulated the infusion protocol used in the
original study, we then used the model to develop an infusion protocol
that would bring the effect site concentration smoothly to the
predetermined level to ensure “breakthrough” without significant
overshoot, and to keep the concentration stable indefinitely. A 100
ng/ml brain concentration was typically achieved during the most intense
period of the DMT experience with a 0.4 mg/kg bolus, and this
concentration was chosen as the desired target concentration for the
infusion. However, lower or higher concentrations can be achieved using
an analogous protocol with modified infusion rates.
We developed our infusion model using the
bolus-elimination-transfer (B.E.T.) methodology, upon which anesthesia
infusion protocols are often based (Coetzee, 2012). An initial bolus, B0, is used to rapidly bring the plasma concentration to the desired level, CT:
The infusion rate is then calculated to equal the sum of the elimination rate, E, and the transfer rate from the central to the peripheral compartment, T.
The sum of E and T gives the overall infusion rate as defined earlier:
Since the model-fitting established that E is dominated by enzymatic clearance, k10 must be reformulated in terms of Michaelis-Menten kinetics:
This gives the maintenance infusion rate, RT, as:
Since the first term in the RT
equation depends only on the plasma concentration, it becomes constant
when a steady state concentration is reached. The exponential term is
only important before steady state is reached, in the initial stage of
the infusion. It then decays to zero. Assuming the steady state
concentration is the desired effect site concentration, CT, the maintenance infusion rate, Rss, can be calculated:
Using the estimated model parameters, this gives a
steady state infusion rate of 0.93 mg/min. However, during the first few
min of the infusion, the exponential term is large; i.e., there is
rapid transfer of drug from the central to the peripheral compartment.
This rate of transfer peaks at 3.3 mg/min, at around 2.3 min, before
declining rapidly. The infusion rate must be set to compensate for this
transfer, being decreased gradually until Rss
is reached. This variable infusion rate is essential to attaining and
maintaining a stable effect site concentration. If the initial rate is
too low following the initial bolus, the effect site concentration
plummets well below that desired and is not maintained. Conversely, if a
high initial infusion rate is maintained, the effect site concentration
continues to increase. It is possible that this accounts for the
relatively high rate of volunteers dropping out of the
Gouzoulis-Mayfrank study (Gouzoulis-Mayfrank et al., 2005).
To examine the possibility of effect site concentration
overshoot, we performed simulations using the Gouzoulis-Mayfrank
infusion protocol: 0.3 mg/kg bolus, followed by an infusion beginning at
1.5 min, at a rate of 0.02 mg/kg/min over 84 min. Figure 4
shows the expected effect site concentration over this infusion period
for a 75 kg subject. The initial bolus produces an effect site
concentration of 80 ng/ml; i.e., a breakthrough dose. Once the infusion
begins, however, the concentration rises steadily, and reaches 150 ng/ml
by the end of the session. This is a very high concentration and is
certain to produce extremely intense effects in almost all individuals.
FIGURE 4
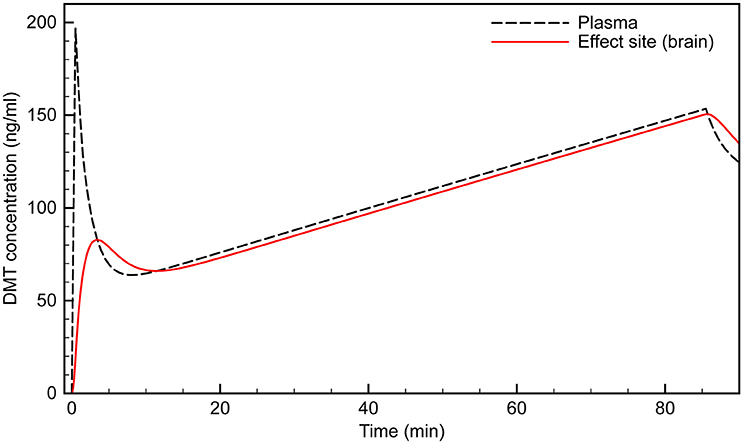
Figure 4. Simulated time course of plasma and effect site DMT concentration using the (Gouzoulis-Mayfrank et al., 2005) protocol.
Using our PK model, we developed an
infusion protocol that maintains an effect site concentration of ~100
ng/ml in a 75 kg subject (Figure 5).
An initial bolus of 25 mg infused over 30 s rapidly brings the effect
site concentration to just over 100 ng/ml. Although the plasma
concentration spikes at over 200 ng/ml, the desired effect site
concentration is reached smoothly with very little overshoot. The
infusion begins at 2 min at a rate of 4.2 mg/min. The infusion is
updated every min, and decreases according to the peripheral transfer
rate decay (the exponential term in the RT
equation). Steady state does not occur until after 20 min of infusion,
after which a constant maintenance infusion rate of 0.93 mg/min is
employed.
FIGURE 5
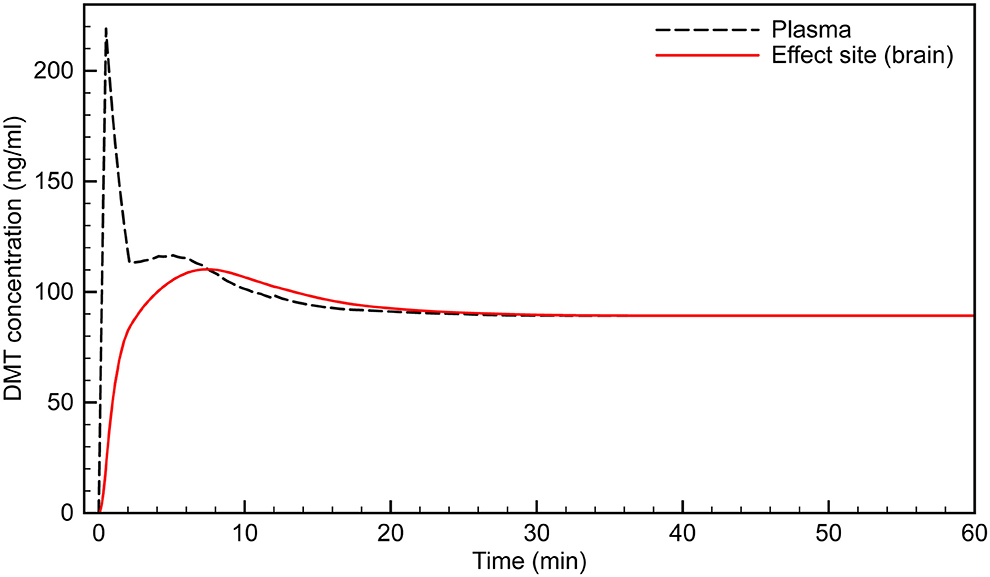
Figure 5. Simulated time course of infusion protocol designed to reach and maintain effect site concentration of ~100 ng/ml.
The blood sample data used in this work was from a previous study (Strassman and Qualls, 1994)
approved by the Scientific Advisory Committee of the General Clinical
Research Center (GCRC) and Human Research Review Committee of the
University of New Mexico School of Medicine, Albuquerque, the New Mexico
State Pharmacy Board, the US Drug Enforcement Administration, and the
US Food and Drug Administration. Witnessed written informed consent was
obtained from all subjects, and confidentiality and anonymity were
maintained throughout the study.
Discussion
The phenomenological content of dream states (Schredl and Hofmann, 2003; Kahan and Laberge, 2011; Thomas et al., 2015) and hallucinations in psychotic disorders have been studied extensively (Jardri et al., 2014; Wilkinson, 2014),
with the aim of deepening our understanding of the structure of normal
and abnormal states of consciousness. However, whilst the endogenous
human hallucinogen DMT reliably and reproducibly generates one of the
most unusual states of consciousness available, its phenomenology has
only begun to be characterized. One of the reasons for this is its short
duration of action. A technology for extending DMT experiences in a
controlled manner beyond what is achievable using bolus administration
therefore would be of great value.
Modern target-controlled infusion protocols employ
algorithms that allow the infusion rate to be calculated and adjusted in
real time, such that the effect site drug concentration can be raised
and lowered in order to control, for example, the level of anesthesia (Bailey and Shafer, 1991; Shafer and Gregg, 1992).
Our analysis highlights the potential of using the target-controlled
infusion methodology for extended DMT sessions. Using time-series blood
sampling data and pharmacokinetic modeling, we propose that the unique
pharmacological characteristics of DMT make it suitable for
administration by target-controlled intravenous infusion. These
characteristics include a rapid and short-acting effect, and lack of
acute tolerance to its subjective effects. Such methods could be used to
control the depth of the experience during a DMT session, moving the
subject into more intense levels of DMT intoxication or lowering them
back into more manageable levels to provide both respite and easier
communication with the research team.
The methodology developed here is the first step toward a
protocol that is ready for use in research subjects. The purpose of
this modeling is to provide a proof-of-principle that the
pharmacokinetic and pharmacodynamic properties of DMT are such that
stable effect site concentrations can be achieved using
target-controlled infusion. More extensive sampling and more detailed
pharmacokinetic modeling are required to establish definitive population
parameters, the extent of inter- and intra-subject variability, and
covariates.
As with any drug administered by target-controlled
infusion, subject covariates including weight, age, gender, and liver
function create significant inter-subject and intra-subject variability
in the dose-concentration response (White et al., 2008).
In this study, the mean coefficients of variation in plasma DMT
concentration across the 0.2 and 0.4 mg/kg groups were 83 and 58%,
respectively. Although this variability appears large, dose-response
coefficients of variation between 40 and 60% for anesthetic agents
(e.g., propofol) administered by bolus injection are typical. However,
the response variability for continuous infusion protocols is always
lower than that observed for bolus injection (Hu et al., 2005).
Even with well-established infusion protocols, plasma drug
concentrations typically deviate 20–30% above or below the target
concentration (Coetzee et al., 1995).
For this reason, most anesthesia infusion protocols undergo a number of
iterations as pharmacokinetic models are updated and refined.
Thus, the variability observed in this initial modeling
study does not preclude the development of a target-controlled infusion
protocol for DMT. In addition, despite the large dose-concentration
variability, the variability in the relationship between the dose and
the subjective response was much lower. The coefficients of variation of
the subjective response scores, as measured by the Hallucinogen Rating
Scale, an instrument designed specifically to assess the DMT effect,
were 46 and 32% for the 0.2 and 0.4 mg/kg groups, respectively (Strassman et al., 1994).
This 45% lower subjective response variability compared to
dose-concentration variability suggests that a broader target
concentration window exists for attainment of the desired subjective
effect than might be predicted from dose-concentration variability
alone. Therefore, the target concentration accuracy typically achieved
with anesthetic agents is likely to be suitable in a DMT infusion
protocol.
The DMT-containing plant-based decoction ayahuasca provides an extended “DMT experience” lasting several hour (Shanon, 2003; Frenopoulo, 2005; Schmidt, 2012). The phenomenology of the ayahuasca state has been the subject of more extensive analyses than that of pure DMT (Shanon, 2005).
However, to render the preparation orally-active, the ayahuasca brew
must contain both a DMT-containing plant as well as one containing a
beta-carboline MAO inhibitor, such as harmaline (McKenna et al., 1984).
Since beta-carbolines themselves possess psychoactive properties and
may potentiate the effects of other psychoactive alkaloids in the plant
mixture (Callaway et al., 1999),
the subjective effects of ayahuasca differ from those of pure DMT.
Furthermore, it is not possible to precisely regulate and maintain the
effect-site DMT concentration with an oral preparation.
There are a number of research questions that a
successful application of target-controlled IV infusion of DMT may
address. For example, the maximum DMT effect may extend further than
what has been previously described in bolus studies. Very high acute
doses of DMT typically produce a delirium, and users are unable to
recall details of the experience. However, this may result from too
rapidly attaining supra-maximal concentrations of drug. Using the method
described here, it may be possible to move the individual gradually
into a greater level of intoxication while maintaining the
characteristic mental clarity associated with fully psychedelic doses.
In addition, this model is applicable to studies of the
neural correlates of the psychedelic state as revealed by modern
functional neuroimaging techniques, which are also of great interest (Carhart-Harris et al., 2016; Speth et al., 2016).
Since such protocols usually require the research subject to be under
the influence of the drug for an extended period of time, our
methodology would benefit these investigations as well.
Finally, there are potential psychotherapeutic
applications. With the resumption of clinical research with psychedelic
drugs, projects confirming and extending early research demonstrating
the benefit of psychedelic drug-assisted psychotherapy are playing a
prominent role. The conditions to which these novel treatments are being
applied include depression (Berman et al., 2000; Aan Het Rot et al., 2010; Buchborn et al., 2014), obsessive-compulsive disorder (Moreno and Delgado, 1997), dysphoric psychological accompaniments of terminal illness (Grof et al., 1973; Grob et al., 2011), prisoner recidivism (Hendricks et al., 2014), and substance abuse disorders—including alcohol (Bogenschutz et al., 2015) and tobacco (Mangini, 1998; Krebs and Johansen, 2012).
All of the psychedelic substances being used in these studies—LSD,
psilocybin, and ayahuasca—exert their effects over the course of 6–12 h,
consistent with their pharmacokinetic profiles.
One of the advantages of the rapid onset and short
duration of intravenous DMT effects is the ability to enter into and
exit out of a highly altered state in short order. The therapeutic
potential of this characteristic of DMT was illustrated by an unexpected
finding in the DMT tolerance study (Strassman et al., 1996).
Normal control volunteers received four fully psychedelic 0.3 mg/kg
doses of DMT at 30 min intervals. During the 10–15 min of relative
lucidity between doses, they were quite capable of describing both the
effects they had just undergone as well as what they anticipated would
be the effects of the subsequent dose(s). The overwhelming effects of a
psychedelic dose of DMT contributed to a heady and dynamic psychological
confluence of self-disclosure, anticipation, anxiety, vulnerability,
and intimacy. In addition, we found that nearly every subject's sessions
contained an ongoing set of themes, or “storyline.” These themes began
with the first dose, evolved over the following two, and resolved and/or
culminated in the fourth. The opportunity provided by talking with a
therapeutically-trained research team during the inter-bolus periods
contributed to the psychological work that these normal volunteers were
able to do. We doubt that this would have been possible if the
volunteers were under the influence of the drug unabatedly for that same
2.5 h period.
This paradigm of a continuous target-controlled infusion
similarly could be turned to therapeutic purposes in a patient
population. Using this model, patients could be “titrated” for both the
duration and intensity of the DMT state that was most useful for
augmenting the psychotherapeutic process.
For example, in the case of working through trauma, re-experiencing the feared stimulus in the altered state might be initiated with induction into a mildly altered state of relatively brief duration. In the course of treatment, a more prolonged and intense altered level of consciousness could be applied to a more extensive working through process, broadening and deepening the therapeutic gains begun with shorter and lighter exposures.
For example, in the case of working through trauma, re-experiencing the feared stimulus in the altered state might be initiated with induction into a mildly altered state of relatively brief duration. In the course of treatment, a more prolonged and intense altered level of consciousness could be applied to a more extensive working through process, broadening and deepening the therapeutic gains begun with shorter and lighter exposures.
In summary, we have described the rationale, and
presented the requisite pharmacokinetic calculations, for the
development of target-controlled intravenous infusion of the powerful
endogenous psychedelic substance, DMT. The successful demonstration of
this model would provide a valuable tool in determining the role of DMT
in normal and altered states of consciousness, and have broad
psycho-heuristic, functional imaging, and clinical applicability.
Author Contributions
AG performed the analyses. RS provided the original blood sample data. AG and RS wrote the paper.
Funding
This work was funded in part by the Okinawa Institute of Science and Technology Graduate University, Okinawa, Japan.
Conflict of Interest Statement
The authors declare that the research was conducted in
the absence of any commercial or financial relationships that could be
construed as a potential conflict of interest.
References
Belleville, R. E.,
Fraser, H. F., Isbell, H., Logan, C. R., and Wikler, A. (1956). Studies
on lysergic acid diethylamide (LSD-25). I. Effects in former morphine
addicts and development of tolerance during chronic intoxication. AMA. Arch. Neurol. Psychiatry 76, 468–478. doi: 10.1001/archneurpsyc.1956.02330290012002
Cozzi, N. V.,
Gopalakrishnan, A., Anderson, L. L., Feih, J. T., Shulgin, A. T., Daley,
P. F., et al. (2009). Dimethyltryptamine and other hallucinogenic
tryptamines exhibit substrate behavior at the serotonin uptake
transporter and the vesicle monoamine transporter. J. Neural Transm. 116, 1591–1599. doi: 10.1007/s00702-009-0308-8
Vollenweider, F.
X., Leenders, K. L., Scharfetter, C., Maguire, P., Stadelmann, O., and
Angst, J. (1997). Positron emission tomography and fluorodeoxyglucose
studies of metabolic hyperfrontality and psychopathology in the
psilocybin model of psychosis. Neuropsychopharmacology 16, 357–372. doi: 10.1016/S0893-133X(96)00246-1
No comments:
Post a Comment